Incidental occurrence of an unusually large mastoid foramen on cone-beam computed tomography and review of the literature
- Affiliations
-
- 1Department of Oral and Maxillofacial Medicine and Diagnostic Sciences, School of Dental Medicine, Case Western Reserve University, Cleveland, OH, USA.
- 2Division of Radiology, University of Pennsylvania School of Dental Medicine, Philadelphia, PA, USA. mmd@upenn.edu
- KMID: 2160156
- DOI: http://doi.org/10.5624/isd.2016.46.1.39
Abstract
- The incidental finding of an enlarged mastoid foramen on the right posterior mastoid region of temporal bone is reported, together with a discussion of its clinical significance. A 67-year-old female underwent the pre-implant assessment of a maxillary left edentulous region. A cone-beam computed tomographic (CBCT) image was acquired and referred for consultation. Axial CBCT slices revealed a unilateral, well-defined, noncorticated, low-attenuation, transosseous defect posterior to the mastoid air cells in the right temporal bone. The borders of the osseous defect were smooth and continuous. No other radiographic signs suggestive of erosion or sclerosis were noted in the vicinity. The density within the defect was homogenous and consistent with a foramen and/or soft tissue. The patient's history and physical examination revealed no significant medical issues, and she was referred to a neuroradiologist for a second opinion. The diagnosis of an enlarged mastoid foramen was made and the patient was reassured.
MeSH Terms
Figure
-
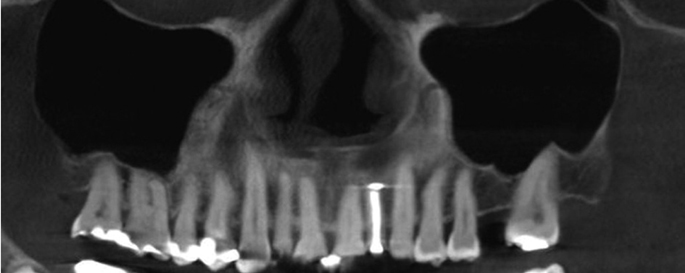
Fig. 1 Cone beam CT panoramic reconstruction of the maxilla shows a missing maxillary left first molar as well as missing third molars bilaterally. The maxillary sinuses are well pneumatized bilaterally.
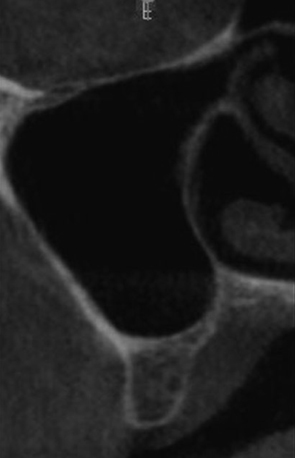
Fig. 2 An orthogonal section of the edentulous area in the region of the left maxillary first molar showing the residual bone in the region, the vicinity of both maxillary sinuses, and the nasal fossa.
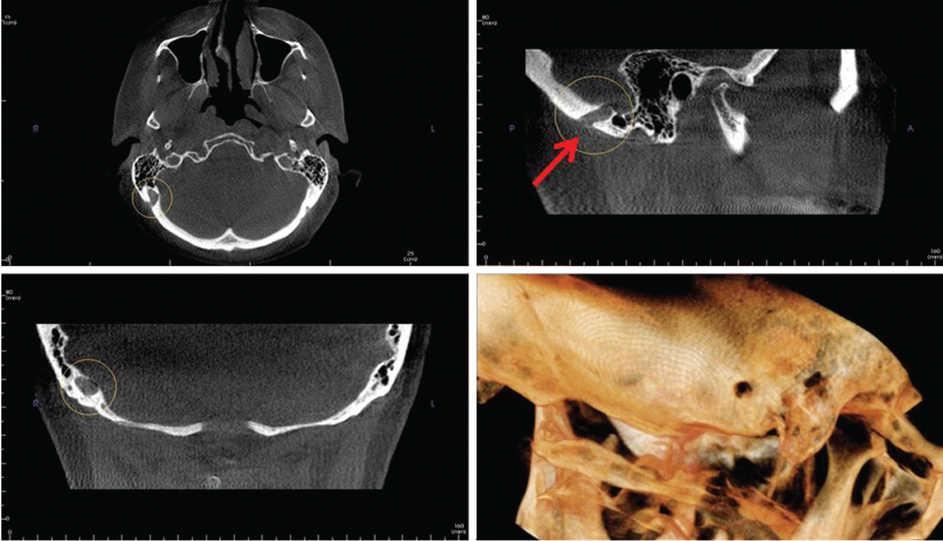
Fig. 3 Cone beam CT multiplanar reconstruction images show an enlarged right mastoid emissary foramen. Axial (top left), sagittal (top right with arrow pointing to the foramen), coronal (bottom left) and three-dimensional volume rendering views (bottom right) demonstrate this anatomical variation.

Fig. 4 Three-dimensional volume rendering shows the large mastoid foramen on the right side (arrow).

Fig. 5 Axial cone beam CT image demonstrates the large right mastoid foramen and a smaller left mastoid foramen (arrowhead).

Fig. 6 Sagittal image of the right mastoid region shows the mastoid foramen measurements (11.2×7.2 mm).
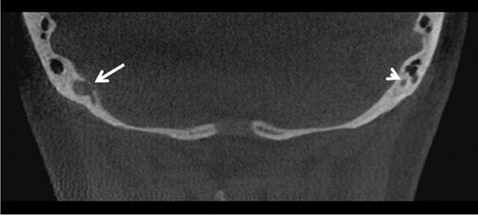
Fig. 7 Intracranial side of the right mastoid foramen (arrow). Note the small mastoid foramen on the left side (arrowhead).
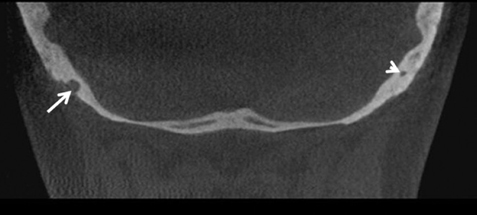
Fig. 8 Extracranial side of the right mastoid foramen (arrow). The smaller left mastoid foramen is still noticeable in this section (arrowhead).
Cited by 2 articles
-
Evaluation of canalis basilaris medianus using cone-beam computed tomography
Ali Z. Syed, Samir Zahedpasha, Sonali A. Rathore, Mel Mupparapu
Imaging Sci Dent. 2016;46(2):141-144. doi: 10.5624/isd.2016.46.2.141.Rare finding of Eustachian tube calcifications with cone-beam computed tomography
Ali Z. Syed, Anna Hawkins, Leela Subashini Alluri, Buthainah Jadallah, Kiran Shahid, Michael Landers, Hussein M. Assaf
Imaging Sci Dent. 2017;47(4):275-279. doi: 10.5624/isd.2017.47.4.275.
Reference
-
1. Kim LK, Ahn CS, Fernandes AE. Mastoid emissary vein: anatomy and clinical relevance in plastic & reconstructive surgery. J Plast Reconstr Aesthet Surg. 2014; 67:775–780.2. Cheatle A. The mastoid emissary vein and its surgical importance. Proc R Soc Med. 1925; 18:29–34.
Article3. Louis RG Jr, Loukas M, Wartmann CT, Tubbs RS, Apaydin N, Gupta AA, et al. Clinical anatomy of the mastoid and occipital emissary veins in a large series. Surg Radiol Anat. 2009; 31:139–144.
Article4. Freire AR, Rossi AC, de Oliveira VC, Prado FB, Caria PH, Botacin PR. Emissary foramens of the human skull: anatomical characteristics and its relations with clinical neurosurgery. Int J Morphol. 2013; 31:287–292.
Article5. Reis CV, Deshmukh V, Zabramski JM, Crusius M, Desmukh P, Spetzler RF, et al. Anatomy of the mastoid emissary vein and venous system of the posterior neck region: neurosurgical implications. Neurosurgery. 2007; 61:Suppl 2. 193–201.6. Chauhan NS, Sharma YP, Bhagra T, Sud B. Persistence of multiple emissary veins of posterior fossa with unusual origin of left petrosquamosal sinus from mastoid emissary. Surg Radiol Anat. 2011; 33:827–831.
Article7. Murlimanju BV, Chettiar GK, Prameela MD, Tonse M, Kumar N, Saralaya VV, et al. Mastoid emissary foramina: an anatomical morphological study with discussion on their evolutionary and clinical implications. Anat Cell Biol. 2014; 47:202–206.
Article8. Calligas JP, Todd NW Jr. Hemorrhage from large mastoid emissary vein: pedicled, rotated, indented, periosteal-galeal flap. Laryngoscope. 2014; 124:551–553.
Article9. Lang J Jr, Samii A. Retrosigmoidal approach to the posterior cranial fossa. An anatomical study. Acta Neurochir (Wien). 1991; 111:147–145.
Article10. Pekçevik Y, Pekçevik R. Why should we report posterior fossa emissary veins? Diagn Interv Radiol. 2014; 20:78–81.
Article11. Dawood A, Patel S, Brown J. Cone beam CT in dental practice. Br Dent J. 2009; 207:23–28.
Article12. Quereshy FA, Savell TA, Palomo JM. Applications of cone beam computed tomography in the practice of oral and maxillofacial surgery. J Oral Maxillofac Surg. 2008; 66:791–796.
Article13. Lee SH, Kim SS, Sung KY, Nam EC. Pulsatile tinnitus caused by a dilated mastoid emissary vein. J Korean Med Sci. 2013; 28:628–630.
Article14. Ahmad R, Ali I, Naikoo GM, Choo NA, Jan F. Giant mastoid emissary vein: source of profuse bleeding during mastoid surgery. Indian J Otolaryngol Head Neck Surg. 2011; 63:Suppl 1. 102–103.
Article15. Koesling S, Kunkel P, Schul T. Vascular anomalies, sutures and small canals of the temporal bone on axial CT. Eur J Radiol. 2005; 54:335–343.
Article16. Pekcevik Y, Sahin H, Pekcevik R. Prevalence of clinically important posterior fossa emissary veins on CT angiography. J Neurosci Rural Pract. 2014; 5:135–138.
Article17. Hadeishi H, Yasui N, Suzuki A. Mastoid canal and migrated bone wax in the sigmoid sinus: technical report. Neurosurgery. 1995; 36:1220–1224.18. Cabanac M, Brinnel H. Blood flow in the emissary veins of the human head during hyperthermia. Eur J Appl Physiol Occup Physiol. 1985; 54:172–176.
Article19. Rivet DJ, Goddard JK 3rd, Rich KM, Derdeyn CP. Percutaneous transvenous embolization of a dural arteriovenous fistula through a mastoid emissary vein. Technical note. J Neurosurg. 2006; 105:636–639.20. Boyd GI. The emissary foramina of the cranium in man and the anthropoids. J Anat. 1930; 65:108–121.21. Keskil S, Gözil R, Çalgüner E. Common surgical pitfalls in the skull. Surg Neurol. 2003; 59:228–231.
Article22. Chen Z, Feng H, Zhu G, Wu N, Lin J. Anomalous intracranial venous drainage associated with basal ganglia calcification. AJNR Am J Neuroradiol. 2007; 28:22–24.23. Marsot-Dupuch K, Gayet-Delacroix M, Elmaleh-Berges M, Bonneville F, Lasjaunias P. The petrosquamosal sinus: CT and MR findings of a rare emisssary vein. AJNR Am J Neuroradiol. 2001; 22:1186–1193.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Foramen transversarium enlargement caused by vertebral artery tortuosity: Diagnosis with cone-beam computed tomography and magnetic resonance angiography
- Anatomical structure of lingual foramen in cone beam computed tomography
- Multiple intraosseous cervical pneumatocysts: A case report of a rare incidental finding on cone-beam computed tomography
- Accessory mental foramen: A rare anatomical variation detected by cone-beam computed tomography
- Fossa navicularis magna detection on cone-beam computed tomography
