Yonsei Med J.
2005 Feb;46(1):66-72. 10.3349/ymj.2005.46.1.66.
Perioperative Anticoagulation in Patients with Mechanical Heart Valves Undergoing Elective Surgery: Results of a Survey Conducted among Korean Physicians
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Pochon CHA University, Sungnam, Korea. doh@cha.ac.kr
- 2Department of Preventive Medicine, College of Medicine, Pochon CHA University, Sungnam, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, College of Medicine, Pochon CHA University, Sungnam, Korea.
- 4Department of Internal Medicine, College of Medicine, Seoul National University, Seoul, Korea.
- 5University of New Mexico, Albuquerque, USA.
- 6McMaster University, Hamilton, Canada.
- 7University of Insubria, Varese, Italy.
- KMID: 2158114
- DOI: http://doi.org/10.3349/ymj.2005.46.1.66
Abstract
- The optimal perioperative anticoagulation management in patients on warfarin therapy is poorly defined due to the lack of randomized trials. Because guidelines are heterogeneous, it was hypothesized that "treatment strategies are not uniform in clinical practice". Between February 2003 and May 2003, a questionnaire with 4 different clinical scenarios was distributed to physicians by e-mail, or direct contact was made by a survey monitor. Two scenarios described the cases of patients with a mechanical heart valve (MHV) in the mitral position, with additional risk factors for a systemic embolism; one undergoing major (scenario 1) and the other minor surgery (scenario 3). Two scenarios described patients with an aortic MHV; one undergoing major (scenario 2) and the other minor (scenario 4) surgery. Different preoperative and postoperative management options were offered. The treatment options for all scenarios were the same. Of the 90 questionnaires distributed, 52 (57.8%) were returned. Hospitalization for full-dose intravenous unfractionated heparin (IV UH) was the most commonly selected strategy in the preoperative phase for scenarios 1 (59%), 2 (42%) and 3 (44%). In scenario 4, 34% chose IV UH. Outpatient, full- dose, subcutaneous UH or low-molecular-weight heparin (LMWH) was the most selected option in the postoperative phase for all scenarios, with the exception of number 4 (52.9% in scenario 1, 34% in scenario 2, 32%, in scenario 3 and 28% in scenario 4). Even among expert clinicians, the management of perioperative anticoagulation is heterogeneous. In particular, the definition of risk categories and the optimal intensity of antithrombotic drugs need to be defined by well-designed prospective studies.
MeSH Terms
Figure
-
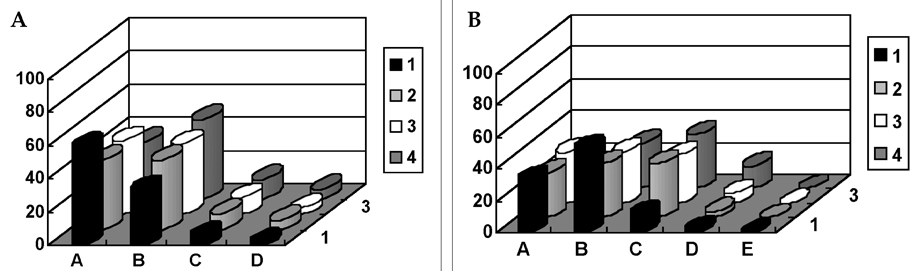
Fig. 1 Preoperative (A) and postoperative (B) anticoagulation management preferences of Korean physicians. 1, 2, 3 and 4 represent the clinical scenarios described in Table 1. A, B, C, D and E represent the anticoagulant options described in Table 2.
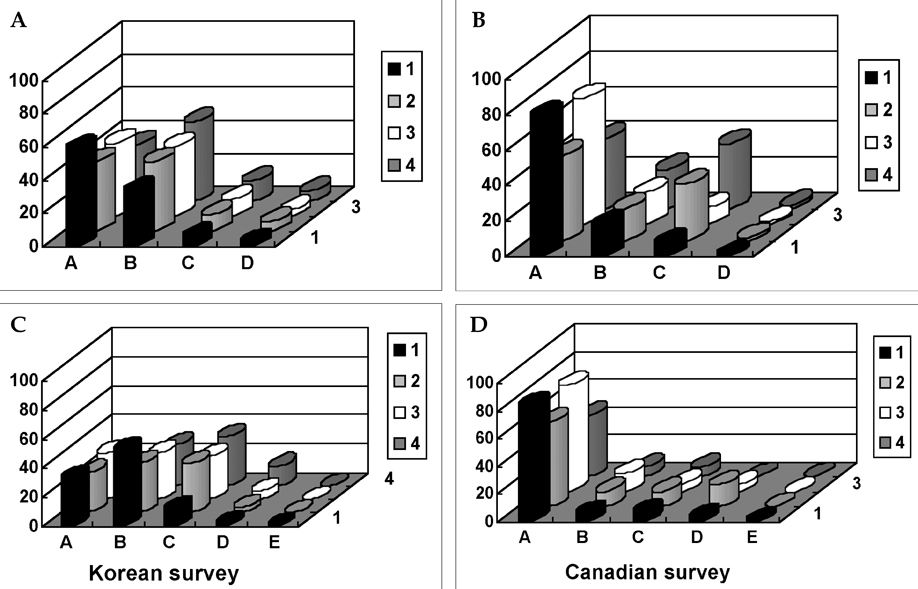
Fig. 2 Comparison of preoperative (A, upper panels) and postoperative (B, lower panels) anticoagulation management preferences of Korean and Canadian physicians. 1, 2, 3 and 4 represent the clinical scenarios described in Table 1. A, B, C, D and E represent the anticoagulant options described in Table 2.
Reference
-
1. Kearon C. Perioperative management of long-term anticoagulation. Semin Thromb Hemost. 1998. 24:Suppl 1. 77–83.2. Bonow RO, Carabello B, de Leon AC Jr, Edmunds LH Jr, Fedderly BJ, Fareed MD, et al. Guidelines for the management of patients with valvular heart disease: executive summary. A report of the American College of Cardiology/American Heart Association Task force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). Circulation. 1998. 98:1949–1984.3. Ansell J, Hirsh J, Dalen J, Bussy H, Anderson D, Poller L, et al. Managing oral anticoagulant therapy. Chest. 2001. 119:22S–38S.4. Douketis JD. Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: a practical guide for clinicians. Thromb Res. 2003. 108:3–13.5. Baudo F, Mostarda G, Boniardi M, et al. The management of patients on long term oral anticoagulant therapy undergoing surgery. Haematologica. 2002. 87:Suppl 2. 48–50.6. Prisco D, Barcellona D, Baudo F, Berretini M, Cianarella N, Cosni B, et al. A guide to oral anticoagulant treatment. Recommendations of the Italian Federation of Anticoagulation Clinics (FCSA). Haematologica. 2003. 88:Suppl 2. 39–41.7. Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med. 1997. 336:1506–1511.8. Turpie AGG, Ageno W. Yusuf S, Cairns JA, Camm AJ, Fallen EL, Gersh BJ, editors. Antithrombotic therapy after heart valve replacement. Evidence based cardiology. 2003. Second Edition. London: BMJ Books;832–836.9. Douketis JD, Crowther MA, Cherian SS, Kearon CB. Physician preferences for perioperative anticoagulation in patients with a mechanical heart valve who are undergoing elective noncardiac surgery. Chest. 1999. 116:1240–1246.10. Acar J, Iung B, Boissel JP, Samama MM, Michel PL, Teppe JP, et al. AREVA: multicenter randomised comparison of low-dose versus standard-dose anticoagulation in patients with mechanical prosthetic heart valves. Circulation. 1996. 94:2107–2112.11. Horstkotte D, Schulte HD, Birks W, Strauer BE. Lower intensity anticoagulation therapy results in lower complication rates with the St. Jude Medical Prosthesis. J Thorac Cardiovasc Surg. 1994. 107:1136–1145.12. Akins CW. Long term results with the Medtronic-Hall valvular prosthesis. Ann Thorac Surg. 1996. 61:806–813.13. Stein PD, Alpert JS, Bussey HI, Dalen JE, Turpie AGG. Antithrombotic therapy in patients with mechanical or biological prosthetic heart valves. Chest. 2001. 119:220S–227S.14. Dolovich LR, Ginsberg JS, Douketis JD, Holbrook AM, Cheah G. A meta-analysis comparing low-molecular-weight heparins with unfractionated heparin in the treatment of venous thromboembolism; examining some unanswered questions regarding location of treatment, product type, and dosing frequency. Arch Intern Med. 2000. 160:181–188.15. Spyropoulos AC, Turpie AGG, Dunn A, Spandorfer J. Regimen Investigators. Clinical outcomes with the use of unfractionated heparin or low-molecular-weight heparin as perioperative bridging therapy in patients on long-term oral anticoagulants: Rationale, objectives, and design of a large, long-term study (REGIMEN).[abstract]. Thromb Haemost. 2003. Suppl. poster #1858.16. Garcia D, Rich JS, Libby E. Bridging therapy for mechanical heart valves: a model comparing unfractionated and low-molecular-weight heparin.[abstract]. Thromb Haemost. 2003. Suppl. poster #1880.17. Spyropoulos AC, Frost FJ, Hurley JS, Roberts M. Health care costs and clinical outcomes in patients on chronic oral anticoagulation undergoing perioperative bridging with low-molecular-weight heparin vs unfractionated heparin.[abstract]. Thromb Haemost. 2001. Suppl. poster #1936.18. Johnson J, Turpie AGG. Temporary discontinuation of oral anticoagulants: role of low molecular weight heparin.[abstract]. Thromb Haemost. 2001. Suppl. poster #2323.19. Tinmouth A, Kovacs MJ, Cruickshank M, Morrow BH, Moore PM. Outpatient peri-operative and peri-procedure treatment with dalteparin for chronically anti-coagulated patients at high risk for thromboembolic complications.[abstract]. Thromb Haemost. 1999. 82:Suppl. poster #662.20. Spandorfer JM, Lynch S, Weitz HH, Fertel S, Merli GJ. Use of enoxaparin for the chronically anticoagulated patient before and after procedures. Am J Cardiol. 1999. 84:478–480.21. Arizo A, Casais P, Meschengieser SS, Sanchez Luceros A, Hendler M, Lazzari MA. Prospective study of the use of low molecular weight heparin vs unfractionated heparin as bridging therapy for invasive procedures in patients anticoagulated with acenocoumarol.[abstract]. Thromb Haemost. 2001. Suppl. CD3646.22. Jenkins S, Beaton K, Hart K, Yeo EL. Outpatient reversal of oral anticoagulation with low molecular weight heparin A pilot study.[abstract]. Thromb Haemost. 2001. Suppl. poster #1421.23. Ferreira I, Dos L, Tornos P, Nicolau I, Permanyer-Miralda G, Soler-Soler J. Experience with enoxaparin in patients with mechanical heart valves who must withhold acenocoumarol. Heart. 2003. 89:527–530.24. Kovacs MJ, Kahn S, Solymoss S, Anderson D, Desjardins L, Kearon C, et al. Prospective multicenter trial of bridging therapy with dalteparin for patients who require temporary discontinuation of OAT with prosthetic heart valves or high risk atrial fibrillation. [abstract]. Blood. 2002. 100:Suppl. 149a.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stroke Prevention in Atrial Fibrillation
- Pregnancy in Patients with Prosthetic Heart Valve
- Low-intensity Oral Anticoagulation Versus High-intensity Oral Anticoagulation in Patients with Mechanical Bileaflet Prosthetic Heart Valves
- Peri-procedural Management of Anticoagulation Therapy (cataract eye surgery, dental procedure and gastrointestinal endoscopy)
- Selection and Complications of Prosthetic Heart Valves
