Unilateral Breast Edema: Spectrum of Etiologies and Imaging Appearances
- Affiliations
-
- 1Department of Diagnostic Radiology, Pochon CHA University, College of Medicine, Korea. ekkim@yumc.yonsei.ac.kr
- 2Department of Pathology, Pochon CHA University, College of Medicine, Korea.
- 3Department of Diagnostic Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea.
- 4National Health Insurance Corporation Ilsan Hospital, Koyang, Korea.
- KMID: 2158106
- DOI: http://doi.org/10.3349/ymj.2005.46.1.1
Abstract
- Breast edema is defined as a mammographic pattern of skin thickening, increased parenchymal density, and interstitial marking. It can be caused by benign or malignant diseases, as a result of a tumor in the dermal lymphatics of the breast, lymphatic congestion caused by breast, lymphatic drainage obstruction, or by congestive heart failure. Here we describe several conditions, that cause unilateral breast edema with the aim of familiarizing radiologists with these disease entities.
Keyword
MeSH Terms
Figure
-

Fig. 1 Inflammatory breast cancer in a 40-year-old woman with a palpable mass and erythematous change of the right breast. Mediolateral mammograms show diffuse increased density, trabecular thickening, skin thickening, and a spiculated mass on the right upper portion (arrows).

Fig. 2 Metastasis in a 43-year-old woman with left breast swelling and skin change. The patient had a signet ring cell carcinoma on her stomach. Biopsy specimens of the hypoechoic nodule in the left breast were evaluated microscopically and immunohistochemically, which included estrogen receptor (ER) and gross cystic disease fluid protein-15 (GCDFP-15), for differentiating primary and metastatic breast cancer. However, the immunohistochemical results for ER and GCDFP-15 were negative, indicating a metastatic signet ring cell carcinoma of the breast. A & B, Mediolateral and craniocaudal mammograms show diffuse increased density, trabecular thickening, and skin change without a definite focal mass. C, Sonogram shows diffuse skin and subcutaneous edema and two suspicious hypoechoic nodules in the left upper outer.
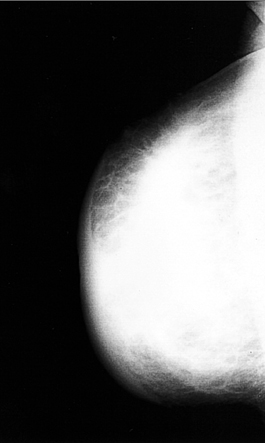
Fig. 3 Breast lymphoma in a 35-year-old woman with a right breast enlargement. Mediolateral oblique mammogram shows diffuse increased opacity throughout the entire right breast with skin thickening.
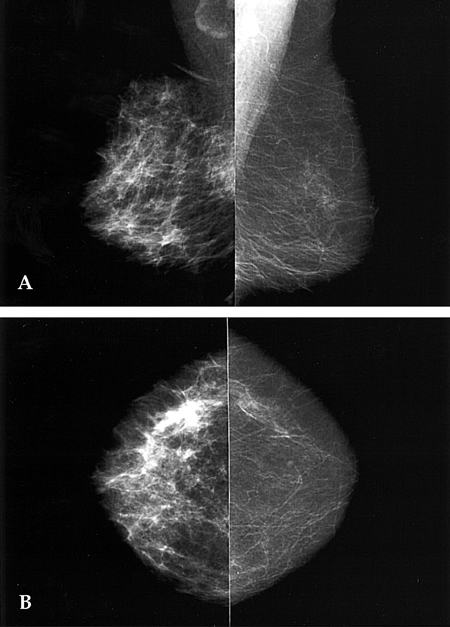
Fig. 4 Mastitis in a 37-year-old woman with breast pain, swelling, and an erythematous change of right breast of 2 weeks duration. After antibiotic treatment the clinical symptoms disappeared. A & B, Mediolateral and craniocaudal mammogram show diffuse skin thickening and accentuated Cooper's ligament.

Fig. 5 Tuberculous abscess in an 81-year-old woman with a painful swelling of the left breast of 2 months duration. A & B, Mediolateral and craniocaudal mammogram show skin thickening, trabecular thickening, and diffuse increased density.
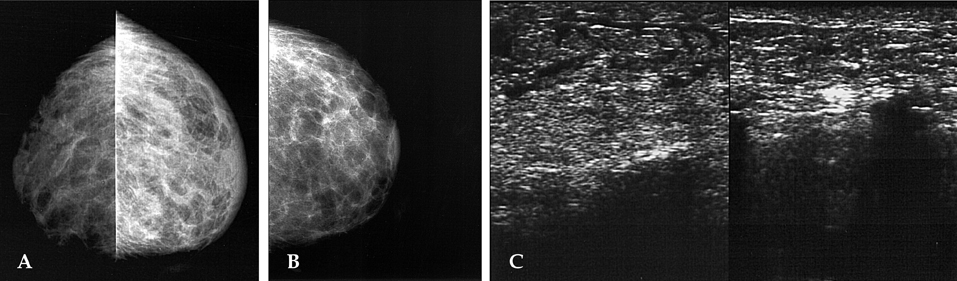
Fig. 6 Congestive heart failure in a 47-year-old woman who complained of dyspnea, dizziness, and a swelling of the left breast. A, Initial craniocaudal mammogram shows diffuse increased density with reticular fascial thickening and marked skin thickening. B, Follow-up left craniocaudal mammogram after 4 weeks of diuretic therapy showing significant resolution of the increased density and skin thickening. C, Sonogram shows marked skin thickening, and an echogenic subcutaneous fat layer with tubular and reticular anechoic structures, suggestive of dilated lymphatics (left), as compared with the normal side (right).

Fig. 7 Post-radiotherapeutic change in a 71-year-old woman due to a poorly differentiated carcinoma of the breast. (A & B) Mediolateral and craniocaudal mammogram show a spiculated mass in upper outer portion of right breast. (C) After partial mastectomy and radiotherapy, this craniocaudal mammography showed diffuse increased density and trabecular and skin thickening as compared to the later 2-year follow-up mammography (D).
Cited by 1 articles
-
Imaging Features of Inflammatory Breast Disorders: A Pictorial Essay
Po Wey Leong, Niketa Chandrakant Chotai, Supriya Kulkarni
Korean J Radiol. 2018;19(1):5-14. doi: 10.3348/kjr.2018.19.1.5.
Reference
-
1. Kim EK, Lee SK, Oh KK. Mammographic and sonographic findings of unilateral breast edema in congestive heart failure: a case report. J Korean Radiol Soc. 1997. 36:1097–1099.2. Swain SM, Lippman M. Bland KI, Copeland EM, editors. Locally advanced breast cancer. The breast: comprehensive management of benign and malignant diseases. 1991. Philadelphia, PA: Saunders;843–862.3. Ellis DL, Teitelbaum SL. Inflammatory carcinoma of the breast: a pathologic definition. Cancer. 1974. 33:1045–1047.4. Dershaw DD, Moore MP, Liberman L, Deutch BM. Inflammatory breast carcinoma: mammographic findings. Radiology. 1994. 190:831–834.5. Tardivon AA, Viala J, Corvellec Rudelli A, Guinebretiere JM, Vanel D. Mammographic patterns of inflammatory breast carcinoma: a retrospective study of 92 cases. Eur J Radiol. 1997. 24:124–130.6. Paulus DD, Libshitz HI. Metastasis to the breast. Radiol Clin North Am. 1982. 20:561–568.7. Chung SY, Oh KK. Imaging findings of metastatic disease to the breast. Yonsei Med J. 2001. 42:497–502.8. Hajdu SL, Urban JA. Cancers metastatic to the breast. Cancer. 1972. 29:1691–1696.9. Vizcaino I, Torregrosa A, Higueras V, Morote V, Cremades A, Torres V, et al. Metastasis to the breast from extramammary malignancies : a report of four cases and a review of literature. Eur Radiol. 2001. 11:1659–1665.10. Petrek JA. Harris JR, Hellman S, Henderson IC, Kinne DW, editors. Lymphoma. Breast diseases. 1991. 2nd. Philadelphia, Pa: Lippincott;806–807.11. Watson AP, Fraser SE. Primary lymphoma of the breast. Australas Radiol. 2000. 44:234–236.12. Liberman L, Giess CS, Dershaw DD, Louie DC, Deutch BM. Non-Hodgkin lymphoma of the breast: imaging characteristics and correlation with histopathologic findings. Radiology. 1994. 192:157–160.13. Schouten JT, Weese JL, Carbone PP. Lymphoma of the breast. Ann Surg. 1981. 194:749–753.14. Dao AH, Adkins RB Jr, Glick AD. Malignant lymphoma of the breast: a review of 13 cases. Am Surg. 1992. 58:792–796.15. Crowe DJ, Helvie MA, Wilson TE. Breast Infection. Mammographic and sonographic findings with clinical correlation. Invest Radiol. 1995. 30:582–587.16. Makanjuola D, Murshid K, Al Sulaimani S, Al Saleh M. Mammographic features of breast tuberculosis: the skin bulge and sinus tract sign. Clin Radiol. 1996. 51:354–358.17. Tabar L, Kett K, Nemeth N. Tuberculosis of the breast. Radiology. 1976. 118:587–589.18. Doyle AJ. Unilateral breast edema in congestive heart failure-a mimic of diffuse carcinoma. Australas Radiol. 1991. 35:274–275.19. Duncan G, Smith R. Cardiac failure mimicking advanced breast carcinoma. Practitioner. 1989. 223:1436–1439.20. Clarke D, Martinez A, Cox RS, Goffinet DR. Breast edema following staging axillary node dissection in patients with breast carcinoma treated by radical radiotherapy. Cancer. 1982. 49:2295–2299.21. Dershaw DD, Shank B, Reisinger S. Mammographic findings after breast cancer treatment with local excision and definitive irradiation. Radiology. 1987. 164:455–461.22. Mendelson EB. Evaluation of the postoperative breast. Radiol Clin North Am. 1992. 30:107–138.23. Gadallah MF, el-Shahawy MA, Campese VM. Unilateral breast enlargement secondary to hemodialysis arteriovenous fistula and subclavian vein occlusion. Nephron. 1993. 63:351–353.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mammographic and Sonographic Findings of Unilateral Breast Edema in Congestive Heart Failure: A Case Report
- CT Appearances of Appendiceal Diseases
- Unilateral pulmonary edema following thoracotomy for the spontaneous pneumothorax
- Reduction mammoplasty as a treatment for symptomatic central venous stenosis
- Ultrasound Spectrum of Papillary Breast Neoplasms
