A Case of Superficial Giant Basal Cell Carcinoma with Satellite Lesions on Scalp
- Affiliations
-
- 1Department of Dermatology, College of Medicine, Korea University, Seoul, Korea. drsshong@medimail.co.kr
- KMID: 2156766
- DOI: http://doi.org/10.5021/ad.2011.23.S1.S111
Abstract
- Giant basal cell carcinoma (BCC), defined as a lesion greater than 5 cm at its largest diameter, is a rare variant of BCC. In contrast to small BCC, giant BCC develops on skin that is not exposed to sunlight, including the back, shoulder, groin and thigh. Most of the histopathologic subtypes of giant BCC are micronodular, morpheaform and nodular, but the superficial subtype is rare. Giant superficial BCC arising on the scalp is extremely rare. We report the case of giant superficial BCC with four satellite lesions on the scalp in a 53-year-old male without predisposing factors.
Keyword
Figure
-

Fig. 1 (A) 6×8 cm sized irregular shaped round pigmented patch with 4 satellite macules on saclp. (B) Tumor shows buds and irregular proliferations of tumor tissue attached to the undersurface of the epidermis (H&E, ×40). (C) The tumor cells have a large, unifrom, oval, nonanaplatic-appearing nucleus with little cytoplasm (H&E, ×100).
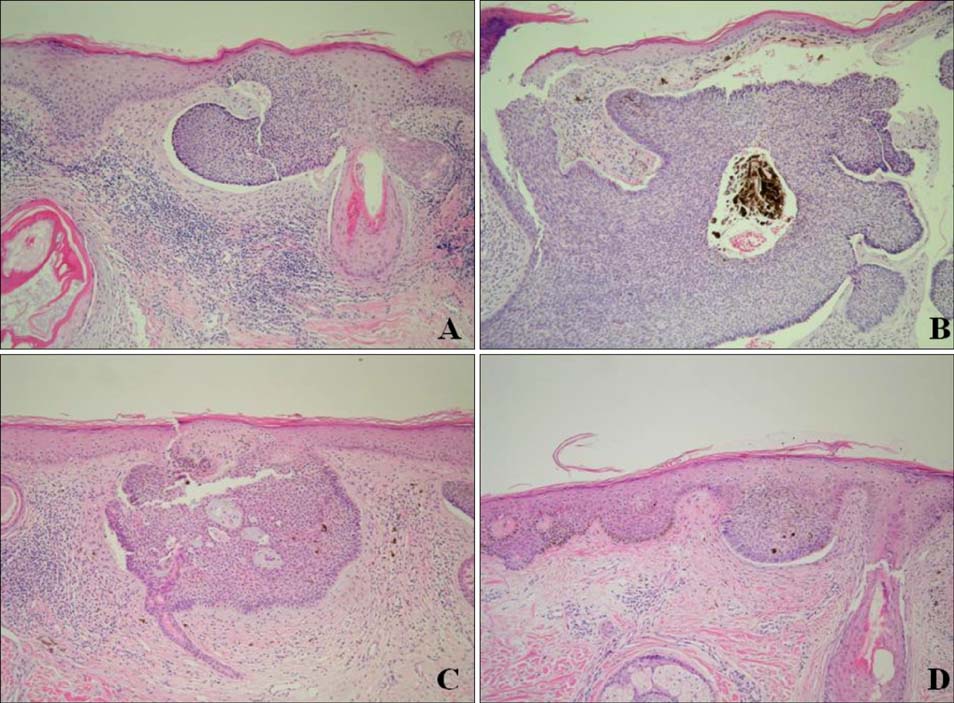
Fig. 2 In satellite lesions from right to left on the scalp. Histopathologic finding showed budding of basaloid cells from the basal layer into the upper dermis, with peripheral palisading and clefting (H&E,×40).

Fig. 3 (A) Two months after the last treatment, lesions revealed only atrophic and hypo-pigmented scar change. (B~D) 7 months later of treatment, follow up biopsies showed only cicatricial fibrosis (B: Center, C: 6 o'clock, D: 12 o'clock).
Reference
-
1. Randle HW. Basal cell carcinoma. Identification and treatment of the high-risk patient. Dermatol Surg. 1996. 22:255–261.
Article2. Randle HW, Roenigk RK, Brodland DG. Giant basal cell carcinoma (T3). Who is at risk? Cancer. 1993. 72:1624–1630.
Article3. Sakamoto GK, Izumi AK. . Giant basal cell carcinoma: report of two cases and review of risk factors. Hawaii Med J. 2005. 64:274–276.4. Lee JH, Park HJ, Kim YC, Cinn YW. A case of giant basal cell carcinoma. Ann Dermatol. 1997. 9:236–238.
Article5. Rossi R, Campolmi P, Giomi B, Massi D, Cappugi P. Giant exophytic basal cell carcinoma treated with radiotherapy. J Eur Acad Dermatol Venereol. 2002. 16:374–376.
Article6. Ceilley RI, Del Rosso JQ. Current modalities and new advances in the treatment of basal cell carcinoma. Int J Dermatol. 2006. 45:489–498.
Article7. Kokoszka A, Scheinfeld N. Evidence-based review of the use of cryosurgery in treatment of basal cell carcinoma. Dermatol Surg. 2003. 29:566–571.
Article8. Gabbi TV, de Lacerda DA, Maruta CW, de Almeida Pimentel ER. Giant superficial basal cell carcinoma treated with cryosurgery. Dermatol Surg. 2008. 34:1441–1442.9. Baust JG, Gage AA, Clarke D, Baust JM, Van Buskirk R. Cryosurgery-a putative approach to molecular-based optimization. Cryobiology. 2004. 48:190–204.
Article10. Hundeiker M, Sebastian G, Bassukas ID, Ernst KJ, Hölzle E. Cryotherapy in dermatology. J Dtsch Dermatol Ges. 2005. 3:1009–1015.11. Majewski S, Marczak M, Mlynarczyk B, Benninghoff B, Jablonska S. Imiquimod is a strong inhibitor of tumor cell-induced angiogenesis. Int J Dermatol. 2005. 44:14–19.
Article12. Bassukas ID, Gamvroulia C, Zioga A, Nomikos K, Fotika C. Cryosurgery during topical imiquimod: a successful combination modality for lentigo maligna. Int J Dermatol. 2008. 47:519–521.
Article
