A Clinical and Histopathological Study of 122 Cases of Dermatofibroma (Benign Fibrous Histiocytoma)
- Affiliations
-
- 1Department of Dermatology, Eulji General Hospital, College of Medicine, Eulji University, Seoul, Korea. ssjmdderma@eulji.ac.kr
- 2Department of Pathology, Eulji General Hospital, College of Medicine, Eulji University, Seoul, Korea.
- KMID: 2156660
- DOI: http://doi.org/10.5021/ad.2011.23.2.185
Abstract
- BACKGROUND
Many variants of dermatofibromas have been described, and being aware of the variants of dermatofibromas is important to avoid misdiagnosis.
OBJECTIVE
We wanted to evaluate the clinical and pathologic characteristics of 122 cases of dermatofibromas.
METHODS
We retrospectively reviewed the medical records and 122 biopsy specimens of 92 patients who were diagnosed with dermatofibroma in the Department of Dermatology at Eulji Hospital of Eulji University between January 2000 and March 2010.
RESULTS
Nearly 80% of the cases occurred between the ages of 20 and 49 years, with an overall predominance of females. Over 70% of the lesions were found on the extremities. The most common histologic variant was a fibrocollagenous dermatofibroma (40.1%). Other variants included histiocytic (13.1%), cellular (11.5%), aneurysmal (7.4%), angiomatous (6.5%), sclerotic (6.5%), monster (4.9%), palisading (1.6%) and keloidal dermatofibromas (0.8%). There were 9 dermatofibromas (7.3%) that were the mixed type with two co-dominant histologic features.
CONCLUSION
The results of this study are consistent with previous reports on the clinical features of dermatofibromas. However, we observed several characteristic subtypes of dermatofibroma and we compared the frequency of the histologic subtypes.
Keyword
MeSH Terms
Figure
-

Fig. 1 The age and gender distribution of the patients.
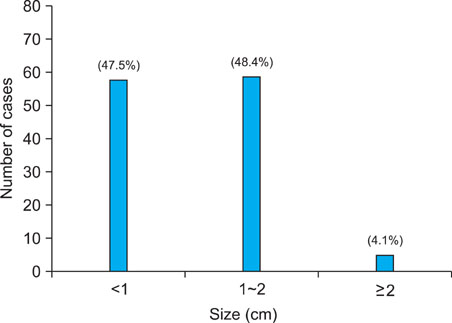
Fig. 2 The size of the lesions.
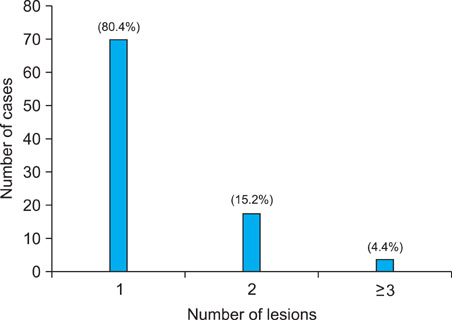
Fig. 3 The number of lesions per each patient.
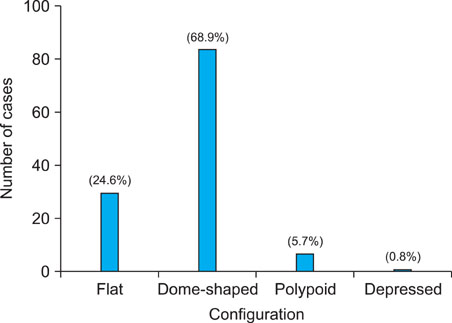
Fig. 4 Configuration of the lesions.

Fig. 5 Distribution of the lesions (%).
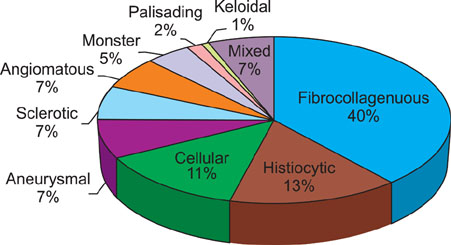
Fig. 6 Classification into the variants of dermatofibroma. The most common histologic variant was a fibrocollagenous dermatofibroma (n=49, 40.1%), followed by histiocytic (n=16, 13.1%), cellular (n=14, 11.5%), aneurysmal (n=9, 7.4%), angiomatous (n=8, 6.5%), sclerotic (n=8, 6.5%), monster (n=6, 4.9%), palisading (n=2, 1.6%) and keloidal dermatofibroma (n=1, 0.8%).
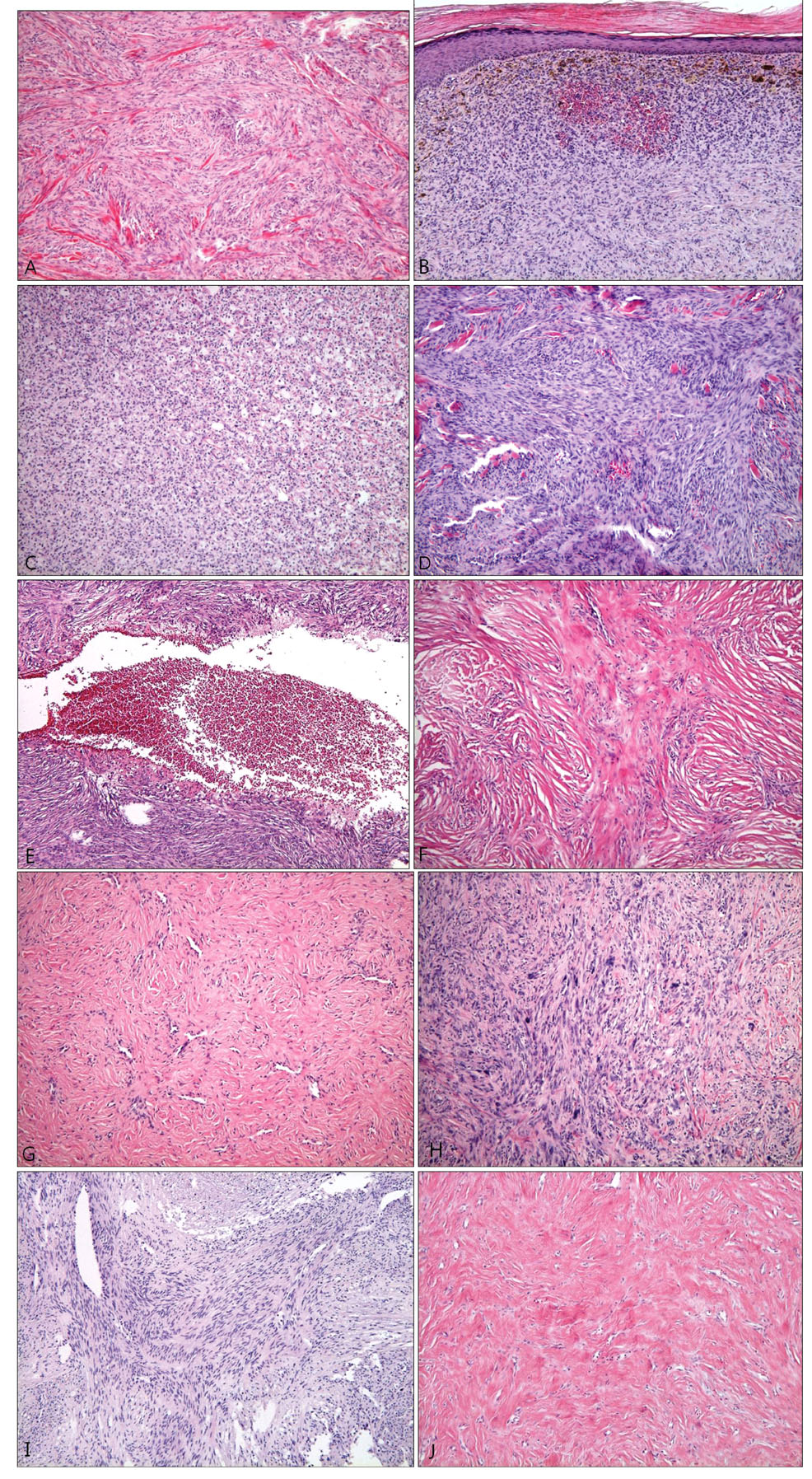
Fig. 7 Various histologic types of dermatofibroma. (A) The fibrocollagenous type shows a predominance of collagen and fibroblasts in a whorled arrangement (H&E, ×100). (B) The histiocytic type shows sheets of histiocytes with many melanophages (H&E, ×100). (C) Foamy histiocytes in the histiocytic type (H&E, ×40). (D) The cellular type showing high cellularity with short fascicular and storiform growth (H&E, ×100). (E) The aneurysmal type is characterized by blood-filled spaces reminiscent of cavernous hemangioma (H&E, ×40). (F) The sclerotic type with marked hyalinized eosinophilic collagen bundles (H&E, ×100). (G) The angiomatous type with numerous small branching vessels in a collagenous stroma (H&E, ×100). (H) The monster type with multinucleate giant cells with large, hyperchromatic, bizarre nuclei (H&E, ×100). (I) The palisading type with verocay-like body in the center of the lesion (H&E, ×100). (J) The keloidal type with broad, thick and irregularly oriented collagen bundles (H&E, ×100).

Fig. 8 Histopathologic features of dermatofibroma. (A) Typical epidermal change of dermatofibroma-induced hyperkeratosis, acanthosis and basal layer hyperpigmentation (H&E, ×100). (B) Lymphoid nodule formation in the cellular type (H&E, ×40). (C) Mucin deposition in the cellular type (alcian blue, ×40).
Cited by 1 articles
-
The Diagnostic Significance of Infiltration Pattern and Perilesional Lymphoid Cell Infiltrate in Dermatofibroma
Min Soo Jang, Jae Woo Baek, Jong Bin Park, Dong Young Kang, Jin Seuk Kang, Sang Tae Kim, Kee Suck Suh
Ann Dermatol. 2012;24(2):228-229. doi: 10.5021/ad.2012.24.2.228.
Reference
-
1. Rahbari H, Mehregan AH. Adnexal displacement and regression in association with histiocytoma (dermatofibroma). J Cutan Pathol. 1985. 12:94–102.
Article2. Requena L, Fariña MC, Fuente C, Piqué E, Olivares M, Martín L, et al. Giant dermatofibroma. A little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994. 30:714–718.3. De Hertogh G, Bergmans G, Molderez C, Sciot R. Cutaneous cellular fibrous histiocytoma metastasizing to the lungs. Histopathology. 2002. 41:85–86.
Article4. Niemi KM. The benign fibrohistiocytic tumours of the skin. Acta Derm Venereol Suppl (Stockh). 1970. 50:Suppl. 63. 1–66.5. Iwata J, Fletcher CD. Lipidized fibrous histiocytoma: clinicopathologic analysis of 22 cases. Am J Dermatopathol. 2000. 22:126–134.6. Weedon D. Weedon's skin pathology. 2010. 3rd ed. Philadelphia: Churchill Livingstone;821–825.7. Santa Cruz DJ, Kyriakos M. Aneurysmal ("angiomatoid") fibrous histiocytoma of the skin. Cancer. 1981. 47:2053–2061.
Article8. Zelger BW, Steiner H, Kutzner H. Clear cell dermatofibroma. Case report of an unusual fibrohistiocytic lesion. Am J Surg Pathol. 1996. 20:483–491.9. Tamada S, Ackerman AB. Dermatofibroma with monster cells. Am J Dermatopathol. 1987. 9:380–387.
Article10. Antal A, Zelger B, Reifenberger J, Niehues T, Feyen O, Megahed M, et al. Multiple eruptive myxoid dermatofibromas: report of first case and review of literature. Br J Dermatol. 2007. 157:382–385.
Article11. Kuo TT, Hu S, Chan HL. Keloidal dermatofibroma: report of 10 cases of a new variant. Am J Surg Pathol. 1998. 22:564–568.12. Schwob VS, Santa Cruz DJ. Palisading cutaneous fibrous histiocytoma. J Cutan Pathol. 1986. 13:403–407.
Article13. Kuo TT, Chan HL. Ossifying dermatofibroma with osteoclast-like giant cells. Am J Dermatopathol. 1994. 16:193–195.
Article14. Wilson Jones E, Cerio R, Smith NP. Epithelioid cell histiocytoma: a new entity. Br J Dermatol. 1989. 120:185–195.
Article15. McKee PH, Calonje E, Granter SR. Pathology of the skin: with clinical correlations. 2005. 3rd ed. Philadelphia: Elsevier Mosby;1742–1752.16. Ahn SK, Lee NH, Kang YC, Choi EH, Hwang SM, Lee SH. Histopathologic and immunohistochemical findings of dermatofibromas according to the clinical features and duration. Korean J Dermatol. 2000. 38:500–505.17. Kim YJ, Seo SJ, Kim MN, Hong CK, Song KY, Ro BI. A clinical and histopathological study of dermatofibromas. Korean J Dermatol. 1996. 34:769–774.18. Vilanova JR, Flint A. The morphological variations of fibrous histiocytomas. J Cutan Pathol. 1974. 1:155–164.
Article19. Sohn IB, Hwang SM, Lee SH, Choi EH, Ahn SK. Dermatofibroma with sclerotic areas resembling a sclerotic fibroma of the skin. J Cutan Pathol. 2002. 29:44–47.
Article20. Kamino H, Jacobson M. Dermatofibroma extending into the subcutaneous tissue. Differential diagnosis from dermatofibrosarcoma protuberans. Am J Surg Pathol. 1990. 14:1156–1164.21. Chang SE, Choi JH, Sung KJ, Moon KC, Koh JK. Subcutaneous dermatofibroma showing a depressed surface. Int J Dermatol. 2001. 40:77–78.
Article22. Schoenfeld RJ. Epidermal proliferations overlying histiocytomas. Arch Dermatol. 1964. 90:266–270.
Article23. Morgan MB, Howard HG, Everett MA. Epithelial induction in dermatofibroma: a role for the epidermal growth factor (EGF) receptor. Am J Dermatopathol. 1997. 19:35–40.
Article24. Barker SM, Winkelmann RK. Inflammatory lymphadenoid reactions with dermatofibroma/histiocytoma. J Cutan Pathol. 1986. 13:222–226.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Deep Benign Fibrous Histiocytoma Showing Multiple Metastases
- A Case of Deep Aneurysmal Benign Fibrous Histiocytoma with Atypical Clinical Features
- Rare experience of keloidal dermatofibroma of forehead
- A Case of Subcutaneous Benign Fibrous Histiocytoma
- Aneurysmal Benign Fibrous Histiocytoma with Atrophic Features
