Symptomatic Pneumocephalus after Spinal Intradural Tumor Surgery
- Affiliations
-
- 1Department of Neurosurgery, Wooridul Spine Hospital, Seoul, Korea. if2000@wooridul.co.kr
- 2Department of Neurosurgery, Uijeongbu Emergency Medical Information Center, Uijeongbu, Korea.
- KMID: 2156159
- DOI: http://doi.org/10.13004/jknts.2008.4.2.101
Abstract
- We report a patient who developed symptomatic pneumocephalus after surgery for a spinal intradural tumor. A 30-year-old man presented with low back pain and leg pain was presented. Magnetic resonance image (MRI) demonstrated an well-demarcated intradural extramedullary tumor at the L3-4. The mass had little adhesion rootlets at its base. So, we achieved en-bloc total resection without any difficulty. The patient had no postoperative problems immediately after the surgery such as cerebrospinal fluid (CSF) leakage. However, he began to suffer from headache and restlessness about 8 hours after sitting position. Computed tomography (CT) scan revealed pneumocephalus in bilateral sylvian cistern and basal cistern. He was successfully managed conservatively. Although not being CSF leakage or fistula, pneumocephalus developed especially after removal of intradural extramedullary tumor in spine. We think that the air might be entrapped into surgical cavity when tumor burden was en-bloc removed. When the patient was in upright position, subarachnoid air migrated from the spine into the brain.
MeSH Terms
Figure
-
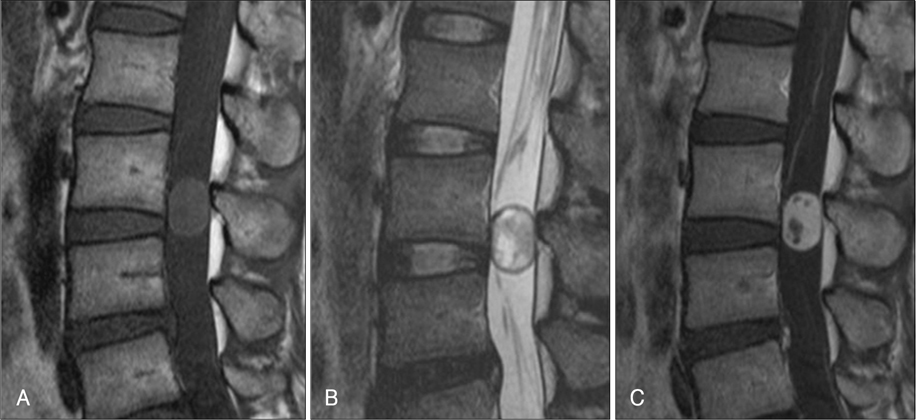
FIGURE 1 Sagittal T1-weighted (A), T2-weighted (B), and contrast enhanced T1-weighted (C) MRI images show a well-defined intradural extramedullary mass at the L3-4. The mass has sharply defined rostral and caudal margins and exhibit intermediate signal intensity. There is a small cyst capping the caudal pole of the tumor. The tumor shows strong homogenous enhancement except for cystic portion.
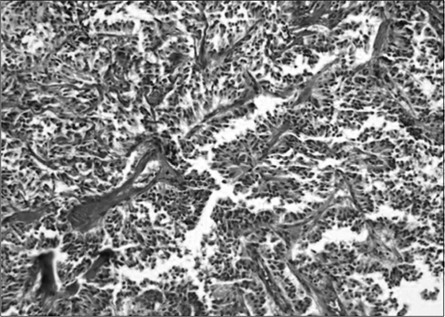
FIGURE 2 Histopathologic findings show typical myxopaillary pattern in the tumor. Cuboidal and columnar tumor cells are arranged like pseudorosette around blood vessel. There is an abundant amount of stroma showing conspicuous myxoid change (H&E, ×200).
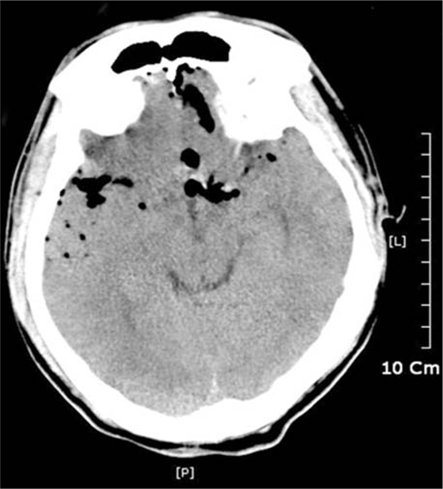
FIGURE 3 6 hours after operation brain CT scan shows pneumocephalus in basal and sylvian cistern.
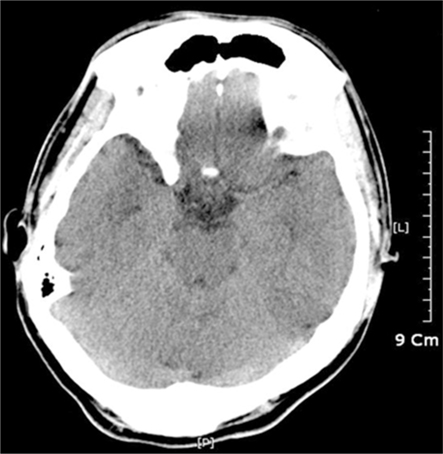
FIGURE 4 Brain CT at 10th postoperative days shows free of air in subarachnoid space.
Cited by 1 articles
-
A Rare Complication of Lumbar Spinal Surgery: Pneumocephalus
Uğur Özdemir
Korean J Neurotrauma. 2017;13(2):176-179. doi: 10.13004/kjnt.2017.13.2.176.
Reference
-
1. Arbit E, Shah J, Bedford R, Carlon G. Tension pneumocephalus: treatment with controlled decompression via a closed water-seal drainage system. Case report. J Neurosurg. 1991; 74:139–142.2. Cihangiroğlu M, Unal B, Ozdemir H, Yildirim H, Ogur E. Pictorial essay: pneumocephalus. Tani Girisim Radyol. 2003; 9:31–35.3. Goh BK, Yeo AW. Traumatic pneumorrhachis. J Trauma. 2005; 58:875–879.
Article4. Guarino AH, Wright NM. Pneumocephalus after a lumbar epidural steroid injection. Pain Physician. 2005; 8:239–241.
Article5. Hong WJ, Yoo CJ, Park CW, Lee SG. Two cases of delayed tension pneumocephalus. J Korean Neurosurg Soc. 2005; 37:59–62.6. Katz DS, Groskin SA, Wasenko JJ. Pneumorachis and pneumocephalus caused by pneumothorax and multiple thoracic vertebral fractures. Clin Imaging. 1994; 18:85–87.
Article7. Kim JW, Lee SH, Lee KS, Ko KC, Kim HK, Khang CG, et al. Post-traumatic tension pneumocephalus of delayed onset. J Korean Neurosurg Soc. 2002; 31:289–292.8. Ladehoff M, Zachow D, Koch C, Nowak G, Echelmeyer A, Arnold H, et al. Cerebellar haemorrhage and tension pneumocephalus after resection of a Pancoast tumour. Acta Neurochir (Wien). 2005; 147:561–564.
Article9. Newbold RG, Wiener MD, Vogler JB 3rd, Martinez S. Traumatic pneumorrhachis. AJR Am J Roentgenol. 1987; 148:615–616.
Article10. Ozturk E, Kantarci M, Karaman K, Basekim CC, Kizilkaya E. Diffuse pneumocephalus associated with infratentorial and supratentorial hemorrhages as a complication of spinal surgery. Acta Radiol. 2006; 47:497–500.
Article11. Pitts LH, Wilson CB, Dedo HH, Weyand R. Pneumocephalus following ventriculoperitoneal shunt. J Neurosurg. 1975; 43:631–633.
Article12. Prabhakar H, Bithal PK, Ghosh I, Dash HH. Pneumorrhachis presenting as quadriplegia following surgery in the prone position. Br J Anaesth. 2006; 97:901–903.
Article13. Sprague A, Poulgrain P. Tension pneumocephalus: a case report and literature review. J Clin Neurosci. 1999; 6:418–424.
Article14. Turgut M, Akyuz O. Symptomatic tension pneumocephalus: an unusual post-operative complication of posterior spinal surgery. J Clin Neurosci. 2007; 14:666–668.
Article15. Turgut N, Turkmen A, Gokkaya S, Hatiboglu MA, Iplikcioglu AC, Altan A. Positive end-expiratory pressure reduces pneumocephalus in spinal intradural tumor surgery. J Neurosurg Anesthesiol. 2007; 19:161–165.
Article16. Uemura K, Meguro K, Matsumura A. Pneumocephalus associated with fracture of thoracic spine: case report. Br J Neurosurg. 1997; 11:253–256.17. Zasler ND. Posttraumatic tension pneumocephalus. J Head Trauma Rehabil. 1999; 14:81–84.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Rare Complication of Lumbar Spinal Surgery: Pneumocephalus
- A Case of Intradural Spinal Lipoma
- Intradural Lipoma in the Lower Thoracic Spinal Cord
- Tension Pneumocephalus after Transsphenoidal Surgery for a Giant Pituitary Tumor: Case Report
- Tension Pneumocephalus after Transsphenoidal Surgery: Report of Two Cases
