Korean J Neurotrauma.
2013 Oct;9(2):52-56. 10.13004/kjnt.2013.9.2.52.
Results of Combined 360-Degree Fusion versus Posterior Fixation Alone for Thoracolumbar Burst Fractures
- Affiliations
-
- 1Department of Neurosurgery, Konyang University Hospital, Daejeon, Korea. naturalspine@gmail.com
- KMID: 2156100
- DOI: http://doi.org/10.13004/kjnt.2013.9.2.52
Abstract
OBJECTIVES
To identify the better option of treatment, we compared the surgical results and efficacy of combined anterior-posterior approach versus posterior fixation alone.
METHODS
During a 10 years period from 2002 to 2011, 111 patients with thoracolumbar burst fracture was surgically managed at our institute. 25 patients were managed by a combined anterior-posterior surgery and 86 patients were managed by posterior fusion alone. Radiographs were repeated at 3, 6, 12 and 24 months after operation. Radiologic outcome was evaluated by measuring Kyphotic angulation and vertebral height and the clinical outcome was evaluated by visual analogue scale (VAS) score comparison.
RESULTS
The average Cobb's angle difference between immediate post operative and last follow up was 15.0degrees in combined 360-degree fusion group and 7.5degrees in posterior surgery alone group. A corrections of vertebral body height between immediate post operative and last follow up was 2.27 mm in 360-degree fusion group while 0.59 mm in posterior fixation group. The VAS score decreased from 8.4 to 2.2 after post operation 24 months in 360-degree fusion group and the posterior surgery alone group decreased 9.3 to 6.2 after post operation 24 months.
CONCLUSION
The combined anterior-posterior approach resulted in less deterioration of the kyphotic angle postoperatively and improvement of vertebral height (sagittal index). Clinical outcome was also better in the combined group.
MeSH Terms
Figure
-
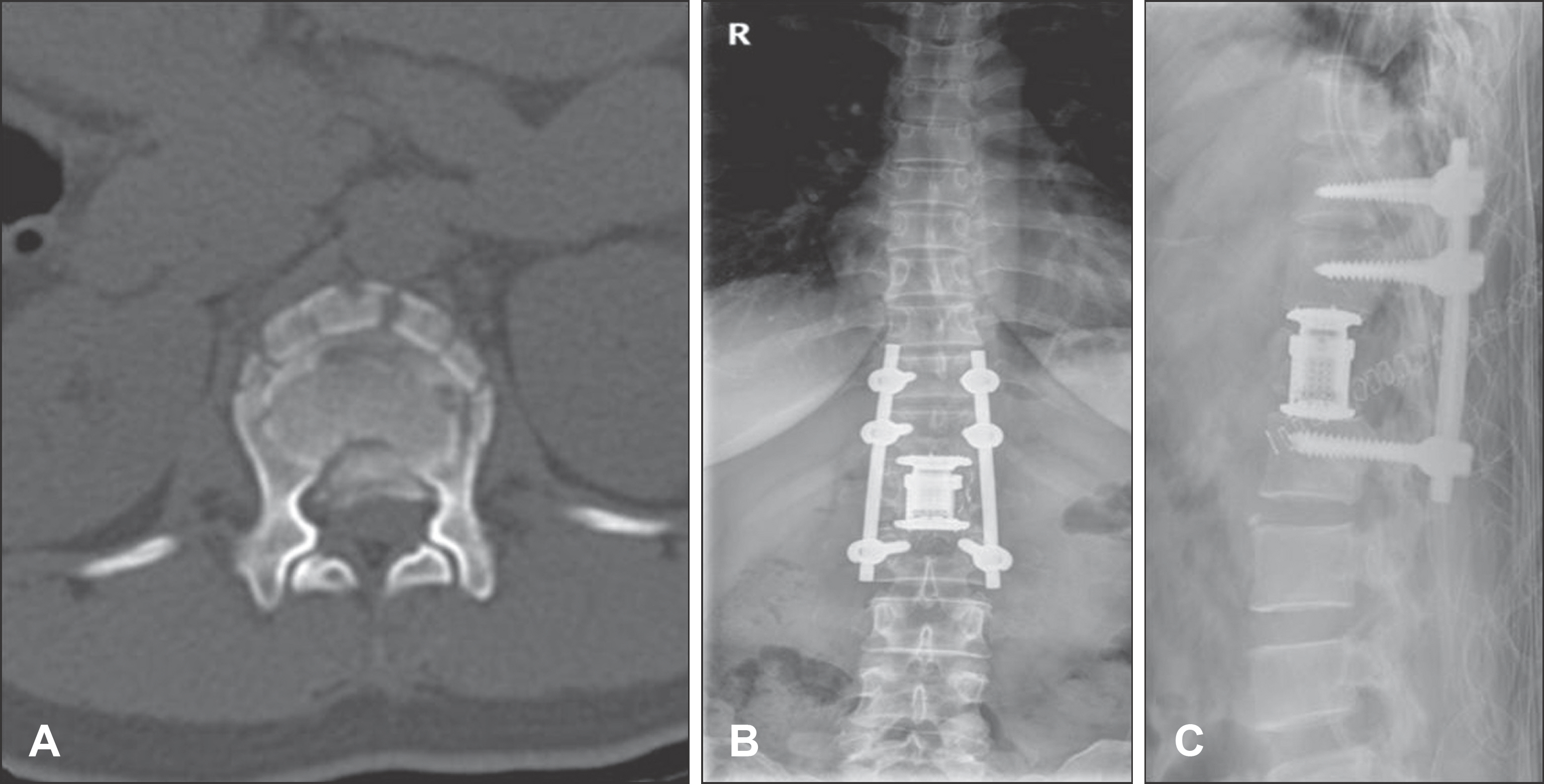
FIGURE 1. A case of thoracolumbar vertebral fracture managed by 360-degree fusion. A: Axial computed tomography scan image of a fractured spine. Bilateral pedicles and facet joints were resected and a cage was inserted. B and C: Plain radiograph showing cage insertion and transpedicular screw fixation.
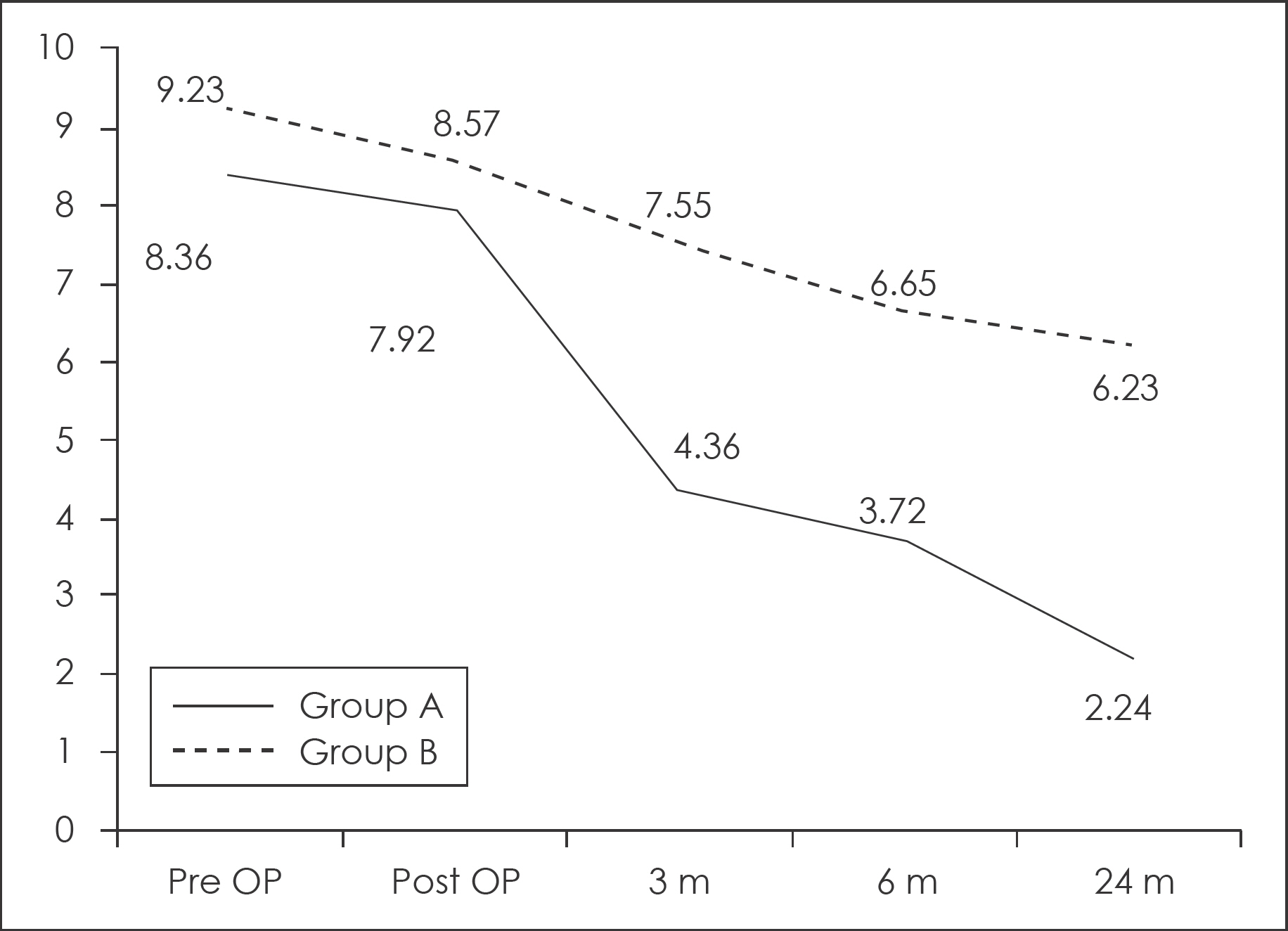
FIGURE 2. Graph showing VAS score at admission, immediate post operation and 3, 6, 24 month after surgery. Group A was 360-degree fusion group and group B was posterior fixation group. VAS: visual analogue scale.
Reference
-
References
1. Aebi M, Etter C, Kehl T, Thalgott J. Stabilization of the lower thoracic and lumbar spine with the internal spinal skeletal fixation system. Indications, techniques, and first results of treatment. Spine (Phila Pa 1976). 12:544–551. 1987.2. Been HD, Bouma GJ. Comparison of two types of surgery for thoracolumbar burst fractures: combined anterior and posterior stabilisation vs. posterior instrumentation only. Acta Neurochir (Wien). 141:349–357. 1999.
Article3. Been HD. Anterior decompression and stabilization of thoracolumbar burst fractures by the use of the Slot-Zielke device. Spine (Phila Pa 1976). 16:70–77. 1991.
Article4. Benzel EC. Short-segment compression instrumentation for selected thoracic and lumbar spine fractures: the short-rod/two-claw technique. J Neurosurg. 79:335–340. 1993.
Article5. Braakman R, Fontijne WP, Zeegers R, Steenbeek JR, Tanghe HL. Neurological deficit in injuries of the thoracic and lumbar spine. A consecutive series of 70 patients. Acta Neurochir (Wien). 111:11–17. 1991.6. Briem D, Lehmann W, Ruecker AH, Windolf J, Rueger JM, Lin-hart W. Factors influencing the quality of life after burst fractures of the thoracolumbar transition. Arch Orthop Trauma Surg. 124:461–468. 2004.
Article7. Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine (Phila Pa 1976) 17 (8 Suppl):S317-S324. 1992.
Article8. Chan DP, Seng NK, Kaan KT. Nonoperative treatment in burst fractures of the lumbar spine (L2-L5) without neurologic deficits. Spine (Phila Pa 1976). 18:320–325. 1993.
Article9. Cotler JM, Vernace JV, Michalski JA. The use of Harrington rods in thoracolumbar fractures. Orthop Clin North Am. 17:87–103. 1986.
Article10. Danisa OA, Shaffrey CI, Jane JA, Whitehill R, Wang GJ, Szabo TA, et al. Surgical approaches for the correction of unstable thoracolumbar burst fractures: a retrospective analysis of treatment outcomes. J Neurosurg. 83:977–983. 1995.
Article11. Denis F, Armstrong GW, Searls K, Matta L. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res:142–149. 1984.
Article12. Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res:65–76. 1984.
Article13. Dick W. The “fixateur interne” as a versatile implant for spine surgery. Spine (Phila Pa 1976). 12:882–900. 1987.14. Dickson JH, Harrington PR, Erwin WD. Results of reduction and stabilization of the severely fractured thoracic and lumbar spine. J Bone Joint Surg Am. 60:799–805. 1978.
Article15. Edwards CC, Levine AM. Early rod-sleeve stabilization of the injured thoracic and lumbar spine. Orthop Clin North Am. 17:121–145. 1986.
Article16. Esses SI, Botsford DJ, Kostuik JP. Evaluation of surgical treatment for burst fractures. Spine (Phila Pa 1976). 15:667–673. 1990.
Article17. Hardaker WT Jr, Cook WA Jr, Friedman AH, Fitch RD. Bilateral transpedicular decompression and Harrington rod stabilization in the management of severe thoracolumbar burst fractures. Spine (Phila Pa 1976). 17:162–171. 1992.
Article18. Hitchon PW, Torner J, Eichholz KM, Beeler SN. Comparison of anterolateral and posterior approaches in the management of thoracolumbar burst fractures. J Neurosurg Spine. 5:117–125. 2006.
Article19. James KS, Wenger KH, Schlegel JD, Dunn HK. Biomechanical evaluation of the stability of thoracolumbar burst fractures. Spine (Phila Pa 1976). 19:1731–1740. 1994.
Article20. Kinoshita H, Nagata Y, Ueda H, Kishi K. Conservative treatment of burst fractures of the thoracolumbar and lumbar spine. Paraplegia. 31:58–67. 1993.
Article21. Knight RQ, Stornelli DP, Chan DP, Devanny JR, Jackson KV. Comparison of operative versus nonoperative treatment of lumbar burst fractures. Clin Orthop Relat Res:112–121. 1993.
Article22. McLain RF. Functional outcomes after surgery for spinal fractures: return to work and activity. Spine (Phila Pa 1976). 29:470–477. ; discussion Z6,. 2004.
Article23. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976). 18:955–970. 1993.24. Oskouian RJ Jr, Shaffrey CI, Whitehill R, Sansur CA, Pouratian N, Kanter AS, et al. Anterior stabilization of three-column thoracolumbar spinal trauma. J Neurosurg Spine. 5:18–25. 2006.
Article25. Sasso RC, Cotler HB. Posterior instrumentation and fusion for unstable fractures and fracture-dislocations of the thoracic and lumbar spine. A comparative study of three fixation devices in 70 patients. Spine (Phila Pa 1976). 18:450–460. 1993.26. Tezeren G, Kuru I. Posterior fixation of thoracolumbar burst fracture: short-segment pedicle fixation versus long-segment instrumentation. J Spinal Disord Tech. 18:485–488. 2005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Posterior Fixation Alone and Supplementation with Posterolateral Fusion in Thoracolumbar Burst Fractures
- Results of Staged 360-Degree Spinal Fusion for Unstable Thoracolumbar Burst Fracture
- Short Segment versus Long Segment Pedicle Screws Fixation in Management of Thoracolumbar Burst Fractures: Meta-Analysis
- Significance of Anterior Support in Thoracolumbar Burst Fracture: Single Stage Interbody Fusion with Transpedicular Screw Fixation Versus Pedicle Screw Fixation with Lamina Onlay Fusion
- Clinical Efficacy of Implant Removal after Posterior Spinal Arthrodesis with Pedicle Screw Fixation for the Thoracolumbar Burst Fractures
