Vascular Map Combined with CT Colonography for Evaluating Candidates for Laparoscopic Colorectal Surgery
- Affiliations
-
- 1Unita Operativa di Radiologia Diagnostica e Interventistica, Azienda Ospedaliera San Paolo, Milan 20142, Italy. nicola.flor@ao-sanpaolo.it
- 2Dipartimento di Scienze della Salute, Universita degli Studi di Milano, Milan 20142, Italy.
- 3Scuola di Specializzazione in Radiodiagnostica, Facolta di Medicina e Chirurgia, Universiti degli Studi di Milano, Milan 20122, Italy.
- 4Unita Operativa di Chirurgia, Azienda Ospedaliera San Paolo, Milan 20142, Italy.
- KMID: 2155555
- DOI: http://doi.org/10.3348/kjr.2015.16.4.821
Abstract
- Contrast-enhanced computed tomography colonography (CE-CTC) is a useful guide for the laparoscopic surgeon to avoid incorrectly removing the colonic segment and the failure to diagnose of synchronous colonic and extra-colonic lesions. Lymph node dissection and vessel ligation under a laparoscopic approach can be time-consuming and can damage vessels and organs. Moreover, mesenteric vessels have extreme variations in terms of their courses and numbers. We describe the benefit of using an abdominal vascular map created by CE-CTC in laparoscopic colorectal surgery candidates. We describe patients with different diseases (colorectal cancer, diverticular disease, and inflammatory bowel disease) who underwent CE-CTC just prior to laparoscopic surgery.
MeSH Terms
Figure
-

Fig. 1 75-year-old man with distal ascending colon cancer (pT3N1a). A. Coronal computed tomography colonography (CTC) image demonstrates stenosing cancer (arrowhead) in distal ascending colon. B. Three-dimensional (3D) endoluminal view confirms stenosis. C. Axial CTC image shows enlarged locoregional lymph node (arrow). D. 3D-fused image shows apple-core wall deformation (arrowhead), presence of right colic artery (RCA), and superior mesenteric vein (SMV) running posterior to arteries. ICA = ileocolic artery, MCA = middle colic artery, SMA = superior mesenteric artery
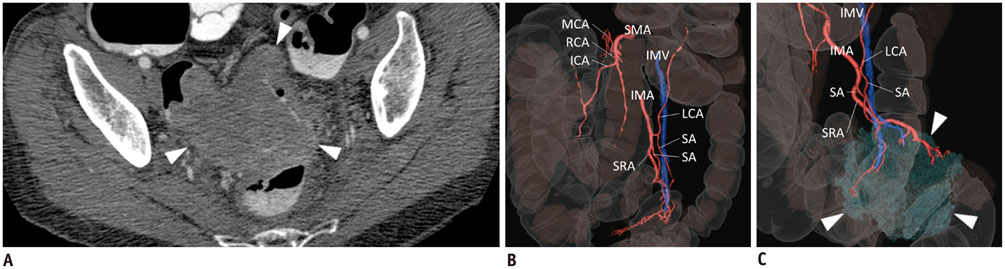
Fig. 2 77-year-old woman with pT3N0 rectal cancer. Axial CTC (A) image shows large stenosing tumor (arrowheads) in proximal rectum. Three-dimensional (3D)-fused images (B, C) demonstrate common origin of left colic artery (LCA) and sigmoid artery (SA), both running anterior to inferior mesenteric vein (IMV); right colic artery (RCA) is also detectable. Lateral view of 3D-fused image (C) shows cancer (arrowheads), its extension, and relationship with feeding vessels. CTC = computed tomography colonography, ICA = ileocolic artery, IMA = inferior mesenteric artery, MCA = middle colic artery, SMA = superior mesenteric artery, SRA = superior rectal artery
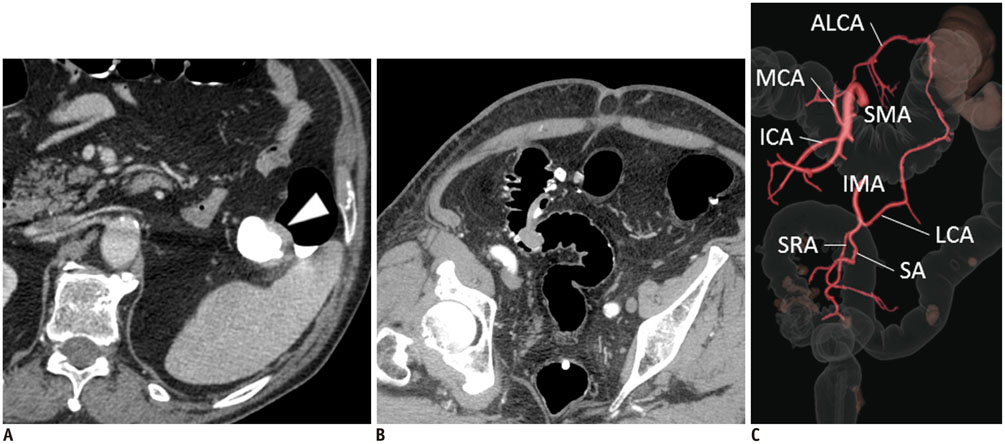
Fig. 3 76-year-old man with colonic cancer. A. Axial computed tomography colonography (CTC) image shows stenosing tumor involving left transverse colon (arrowhead). B. CTC also allows for diagnosis of pedunculated 2-cm synchronous polypoid lesion in sigmoid colon, together with diverticular disease findings. C. Three-dimensional-fused image demonstrates accessory left colic artery (ALCA) branching from middle colic artery (MCA) with separate origin from left colic artery (LCA) and sigmoid arteries (SAs). ICA = ileocolic artery, IMA = inferior mesenteric artery, SMA = superior mesenteric artery, SRA = superior rectal artery
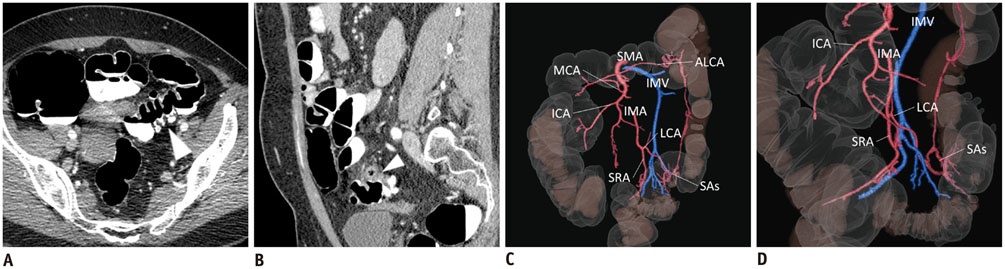
Fig. 4 53-year-old woman with sigmoid chronic diverticulitis was referred for surgery because of symptomatic disease. A, B. Pre-operative computed tomography colonography to assess presence of diverticula (arrowhead in A) and sigmoid colon wall thickening (arrowhead in B) related to disease. C, D. Three-dimensional-fused images demonstrate sigmoid arteries (SAs) branching from left colic artery (LCA) and accessory left colic artery (ALCA) branching from middle colic artery (MCA); LCA and SAs run anteriorly to inferior mesenteric vein (IMV). ICA = ileocolic artery, IMA = inferior mesenteric artery, SMA = superior mesenteric artery, SRA = superior rectal artery
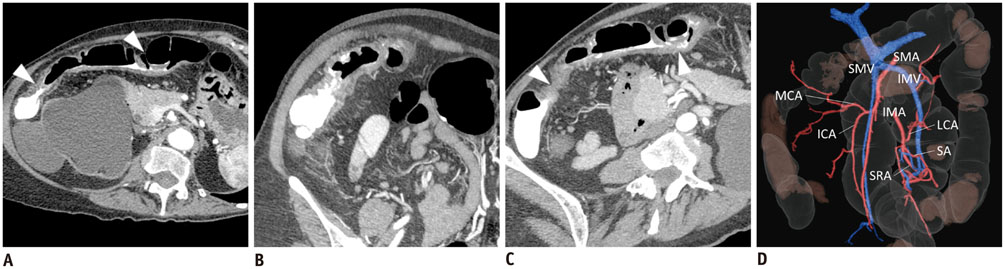
Fig. 5 66-year-old woman with relapsing Crohn's disease. Axial, para-sagittal, and maximum intensity projection reformatted computed tomography colonography (A-C) depict perivisceral "comb sign", enlarged lymph nodes and diffuse colonic wall thickening causing two stenoses (arrowheads in A, C) in transverse colon. Three-dimensional-fused image (D) shows common origin of middle colic artery (MCA) and ileocolic artery (ICA) running posteriorly to superior mesenteric vein (SMV); right colic artery is absent; left colic artery (LCA) runs posteriorly to inferior mesenteric vein (IMV), which drains into SMV. IMA = inferior mesenteric artery, SA = sigmoid artery, SMA = superior mesenteric artery, SRA = superior rectal artery

Fig. 6 32-year-old man with severe Crohn's disease. Axial and coronal computed tomography colonography images (A, B) show involvement of distal ileum and right and transverse colon, causing colonic wall thickening with characteristic "cobblestone" appearance of mucosa (arrowhead), together with perivisceral "comb sign" and enlarged lymph nodes. Three-dimensional-fused images (C, D) demonstrate ileocolic artery (ICA) running posteriorly to superior mesenteric vein (SMV), absence of right colic artery, and inferior mesenteric vein (IMV) draining into SMV, together with characteristic wall thickening (arrowhead). IMA = inferior mesenteric artery, LCA = left colic artery, MCA = middle colic artery, SA = sigmoid artery, SMA = superior mesenteric artery, SMV = superior mesenteric vein, SRA = superior rectal artery
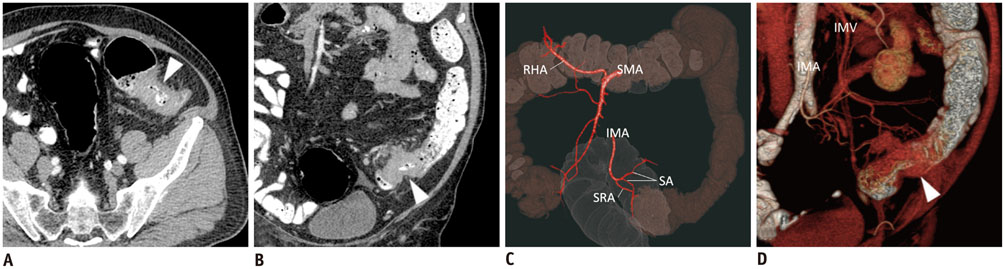
Fig. 7 74-year-old man with sigmoid colon cancer (pT3N1b). Axial and coronal computed tomography colonography images (A, B) show severe sigmoid colon stenosing lesion (arrowhead), preventing adequate bowel preparation. Three-dimensional reconstructions (C, D) demonstrate sigmoid colon lesion (arrowhead in D), sigmoid arteries (SAs) branching directly from inferior mesenteric artery (IMA), running anteriorly to inferior mesenteric vein (IMV); left colic artery is absent; multiple enlarged lymph nodes along tumor feeding vessels are present; moreover, right hepatic artery (RHA) branches from superior mesenteric vein. SMA = superior mesenteric artery, SRA = superior rectal artery
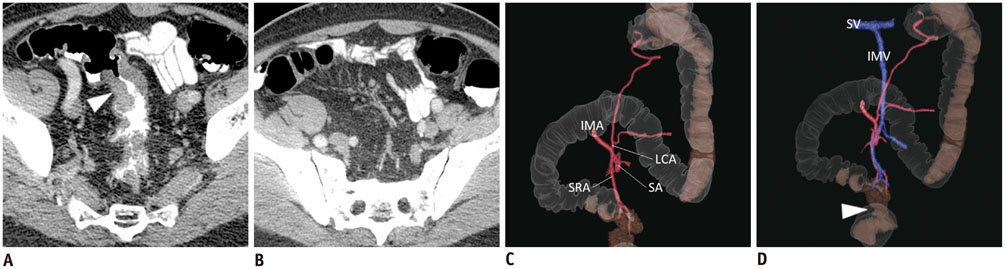
Fig. 8 72-year-old man with sigmoid colon cancer. Axial computed tomography colonography images (A, B) demonstrate sigmoid colon stenosing cancer (arrowhead in A), and enlarged lymph nodes. Three-dimensional-fused images (C, D) show "apple-core" sigmoid colon wall deformity (arrowhead in D), descending branch of left colic artery (LCA), and sigmoid artery (SA) running posteriorly to inferior mesenteric vein (IMV); IMV drains into splenic vein (SV). IMA = inferior mesenteric artery, SRA = superior rectal artery
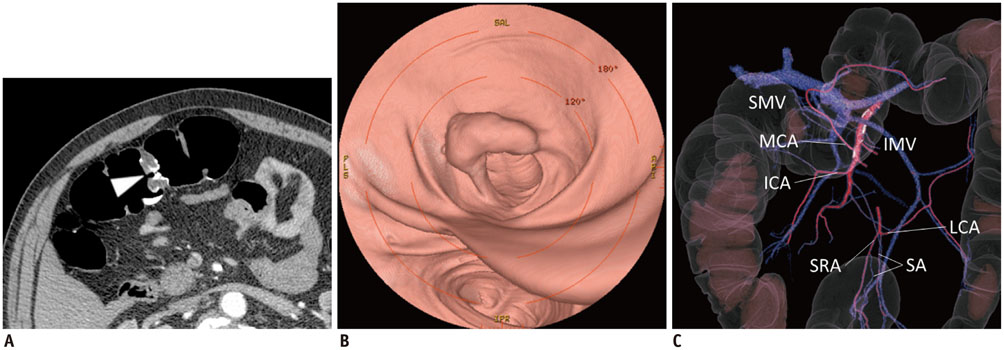
Fig. 9 74-year-old male with 3-cm tubular-villous adenoma and high-grade dysplasia (pTis). Axial and three-dimensional (3D) endoluminal computed tomography colonography (A, B) show vegetating lesion (arrowhead in A) in transverse colon. 3D-fused image (C) shows that right colic artery is absent and both middle colic artery (MCA) and ileocolic artery (ICA) run anteriorly to superior mesenteric vein (SMV); left colic artery (LCA) runs posteriorly to inferior mesenteric vein (IMV); IMV drains into SMV. SA = sigmoid artery, SRA = superior rectal artery
Reference
-
1. Neri E, Turini F, Cerri F, Faggioni L, Vagli P, Naldini G, et al. Comparison of CT colonography vs. conventional colonoscopy in mapping the segmental location of colon cancer before surgery. Abdom Imaging. 2010; 35:589–595.2. Flor N, Ceretti AP, Mezzanzanica M, Rigamonti P, Peri M, Tresoldi S, et al. Impact of contrast-enhanced computed tomography colonography on laparoscopic surgical planning of colorectal cancer. Abdom Imaging. 2013; 38:1024–1032.3. Park SH, Lee JH, Lee SS, Kim JC, Yu CS, Kim HC, et al. CT colonography for detection and characterisation of synchronous proximal colonic lesions in patients with stenosing colorectal cancer. Gut. 2012; 61:1716–1722.4. Flor N, Rigamonti P, Pisani Ceretti A, Romagnoli S, Balestra F, Sardanelli F, et al. Diverticular disease severity score based on CT colonography. Eur Radiol. 2013; 23:2723–2729.5. Regge D, Neri E, Turini F, Chiara G. Role of CT colonography in inflammatory bowel disease. Eur J Radiol. 2009; 69:404–408.6. Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW Jr, et al. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007; 246:655–662. discussion 662-6647. Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005; 6:477–484.8. Ignjatovic D, Sund S, Stimec B, Bergamaschi R. Vascular relationships in right colectomy for cancer: clinical implications. Tech Coloproctol. 2007; 11:247–250.9. Spasojevic M, Stimec BV, Fasel JF, Terraz S, Ignjatovic D. 3D relations between right colon arteries and the superior mesenteric vein: a preliminary study with multidetector computed tomography. Surg Endosc. 2011; 25:1883–1886.10. Hirai K, Yoshinari D, Ogawa H, Nakazawa S, Takase Y, Tanaka K, et al. Three-dimensional computed tomography for analyzing the vascular anatomy in laparoscopic surgery for right-sided colon cancer. Surg Laparosc Endosc Percutan Tech. 2013; 23:536–539.11. Mari FS, Nigri G, Pancaldi A, De Cecco CN, Gasparrini M, Dall'Oglio A, et al. Role of CT angiography with three-dimensional reconstruction of mesenteric vessels in laparoscopic colorectal resections: a randomized controlled trial. Surg Endosc. 2013; 27:2058–2067.12. Matsuki M, Okuda J, Kanazawa S, Kanamoto T, Inada Y, Tatsugami F, et al. Virtual CT colectomy by three-dimensional imaging using multidetector-row CT for laparoscopic colorectal surgery. Abdom Imaging. 2005; 30:698–708.13. Belizon A, Sardinha CT, Sher ME. Converted laparoscopic colectomy: what are the consequences? Surg Endosc. 2006; 20:947–951.14. Kobayashi M, Morishita S, Okabayashi T, Miyatake K, Okamoto K, Namikawa T, et al. Preoperative assessment of vascular anatomy of inferior mesenteric artery by volume-rendered 3D-CT for laparoscopic lymph node dissection with left colic artery preservation in lower sigmoid and rectal cancer. World J Gastroenterol. 2006; 12:553–555.15. Horton KM, Fishman EK. Volume-rendered 3D CT of the mesenteric vasculature: normal anatomy, anatomic variants, and pathologic conditions. Radiographics. 2002; 22:161–172.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of CT Colonography in the Detection of Colorectal Polypoid Lesions
- Diagnostic Performance of CT Colonography for the Detection of Colorectal Polyps
- A Comparison of Patient Acceptance and Preferences Between CT Colonography and Conventional Colonoscopy in Colorectal Cancer Screening
- Virtual CT Colonoscopy and Virtual CT Barium Enema using Multidetector-row CT
- Utility of CT colonography in detecting colon polyps as a colon cancer screen
