Right Ventricular Cardiomyopathy Meeting the Arrhythmogenic Right Ventricular Dysplasia Revised Criteria? Don't Forget Sarcoidosis!
- Affiliations
-
- 1Department of Radiology, Leiden University Medical Center, Leiden 2333 ZA, The Netherlands. l.j.m.kroft@lumc.nl
- 2Department of Pathology, Leiden University Medical Center, Leiden 2333 ZA, The Netherlands.
- 3Department of Radiology, Hospital General Universitario Gregorio Maranon, Madrid 28007, Spain.
- 4Department of Cardiology, Leiden University Medical Center, Leiden 2333 ZA, The Netherlands.
- KMID: 2155539
- DOI: http://doi.org/10.3348/kjr.2015.16.3.668
Abstract
- A 53-year-old woman was referred for ventricular fibrillation with resuscitation. A CT-angiography showed signs of a right ventricular enlargement without obvious cause. A cardiac MRI demonstrated a dilated and hypokinetic right ventricle with extensive late gadolinium enhancement. Arrhythmogenic right ventricular dysplasia (ARVD) was suspected according to the "revised ARVD task force criteria". An endomyocardial biopsy was inconclusive. The patient developed purulent pericarditis after epicardial ablation therapy and died of toxic shock syndrome. The post-mortem pathologic examination demonstrated sarcoidosis involving the heart, lungs, and thyroid gland.
Keyword
MeSH Terms
Figure
-
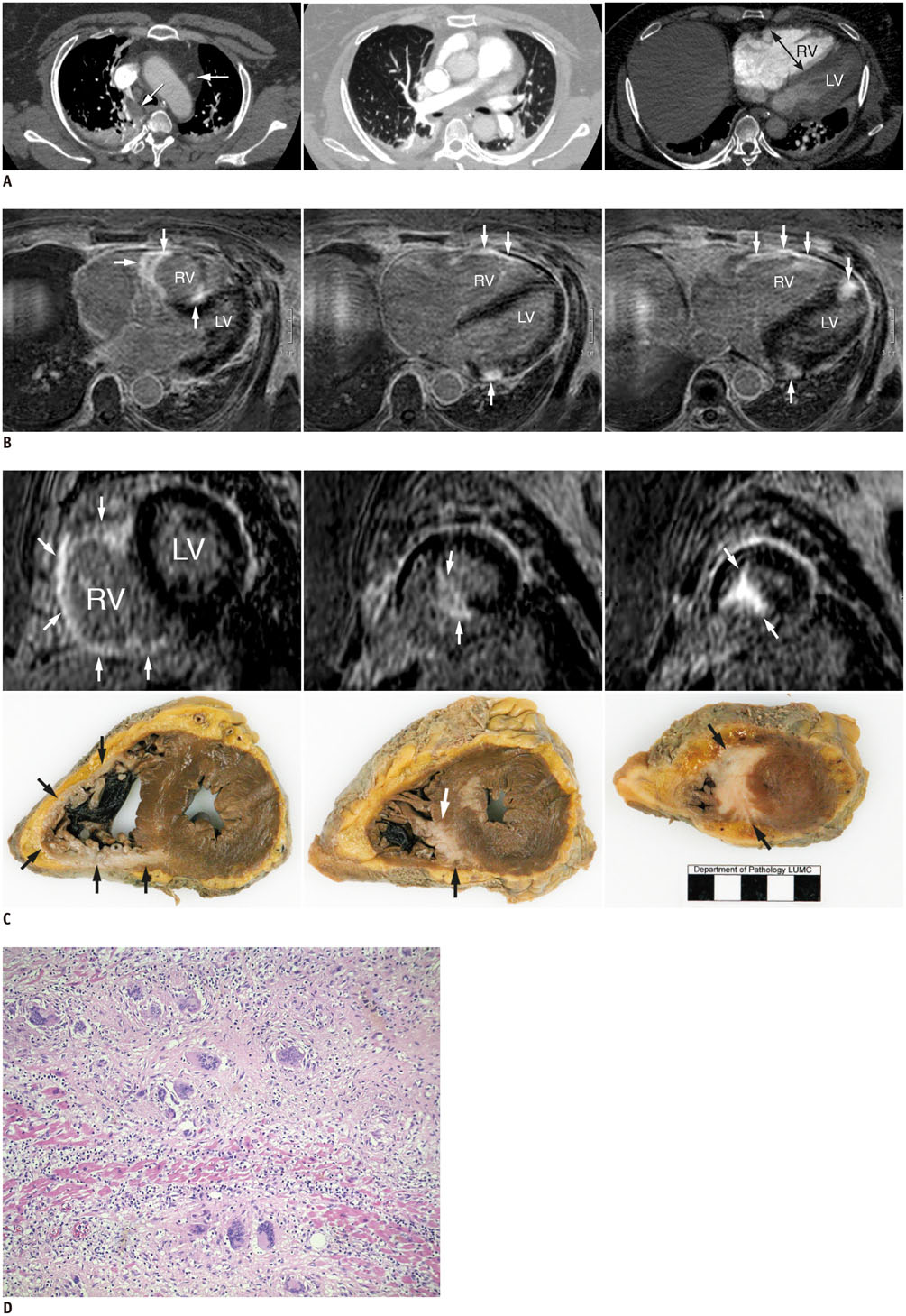
Fig. 1 Cardiac sarcoidosis mimicking arrhythmogenic right ventricular dysplasia in 53-year-old woman. A. Pulmonary CT angiography on admission. Slightly enlarged mediastinal lymph nodes, aspecific finding (arrows, left panel). Bilateral dependent atelectasis but no other pulmonary abnormalities and no pulmonary embolism (left and middle panel). Enlarged right heart, with bowing of interventricular septum towards LV (right panel). B. MRI in axial orientation. Upper level (left panel), middle level (middle panel), and lower level (right panel) MRI showing bright LGE (arrows) in large parts of RV and patchy subepicardial LGE in interventricular septum and LV. LGE = late gadolinium enhancement, LV = left ventricle, RV = right ventricle C. Short-axis MRI images (upper row) compared with gross anatomic sections (lower row). Note perfect correlation between high signal LGE spots (arrows) on MRI at RV wall and apical septum and sarcoidosis granuloma (arrows) on pathology. Base (left panels), mid-ventricular (middle panels), and apex (right panels). D. Histology showing infiltration of histiocytes between myocardial fibers with formation of confluent granulomas and multinucleated giant cells, diagnostic for sarcoidosis (hematoxylin and eosin stain, × 100). Fibrosis and sparse lymphocytic infiltration are present. LGE = late gadolinium enhancement, LV = left ventricle, RV = right ventricle
Reference
-
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007; 357:2153–2165.2. Mantini N, Williams B Jr, Stewart J, Rubinsztain L, Kacharava A. Cardiac sarcoid: a clinician's review on how to approach the patient with cardiac sarcoid. Clin Cardiol. 2012; 35:410–415.3. Roberts WC, McAllister HA Jr, Ferrans VJ. Sarcoidosis of the heart. A clinicopathologic study of 35 necropsy patients (group 1) and review of 78 previously described necropsy patients (group 11). Am J Med. 1977; 63:86–108.4. Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, Fontaliran F, et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol. 1997; 30:1512–1520.5. Lorenz CH, Walker ES, Morgan VL, Klein SS, Graham TP Jr. Normal human right and left ventricular mass, systolic function, and gender differences by cine magnetic resonance imaging. J Cardiovasc Magn Reson. 1999; 1:7–21.6. Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation. 2010; 121:1533–1541.7. Lagana SM, Parwani AV, Nichols LC. Cardiac sarcoidosis: a pathology-focused review. Arch Pathol Lab Med. 2010; 134:1039–1046.8. Yared K, Johri AM, Soni AV, Johnson M, Alkasab T, Cury RC, et al. Cardiac sarcoidosis imitating arrhythmogenic right ventricular dysplasia. Circulation. 2008; 118:e113–e115.9. Vasaiwala SC, Finn C, Delpriore J, Leya F, Gagermeier J, Akar JG, et al. Prospective study of cardiac sarcoid mimicking arrhythmogenic right ventricular dysplasia. J Cardiovasc Electrophysiol. 2009; 20:473–476.10. Ladyjanskaia GA, Basso C, Hobbelink MG, Kirkels JH, Lahpor JR, Cramer MJ, et al. Sarcoid myocarditis with ventricular tachycardia mimicking ARVD/C. J Cardiovasc Electrophysiol. 2010; 21:94–98.11. Hunold P, Wieneke H, Bruder O, Krueger U, Schlosser T, Erbel R, et al. Late enhancement: a new feature in MRI of arrhythmogenic right ventricular cardiomyopathy? J Cardiovasc Magn Reson. 2005; 7:649–655.12. Santangeli P, Hamilton-Craig C, Dello Russo A, Pieroni M, Casella M, Pelargonio G, et al. Imaging of scar in patients with ventricular arrhythmias of right ventricular origin: cardiac magnetic resonance versus electroanatomic mapping. J Cardiovasc Electrophysiol. 2011; 22:1359–1366.13. Cain MA, Metzl MD, Patel AR, Addetia K, Spencer KT, Sweiss NJ, et al. Cardiac sarcoidosis detected by late gadolinium enhancement and prevalence of atrial arrhythmias. Am J Cardiol. 2014; 113:1556–1560.14. Ordovas KG, Higgins CB. Delayed contrast enhancement on MR images of myocardium: past, present, future. Radiology. 2011; 261:358–374.15. Watanabe E, Kimura F, Nakajima T, Hiroe M, Kasai Y, Nagata M, et al. Late gadolinium enhancement in cardiac sarcoidosis: characteristic magnetic resonance findings and relationship with left ventricular function. J Thorac Imaging. 2013; 28:60–66.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Catheter Ablation of Ventricular Tachycardia/Fibrillation in a Patient with Right Ventricular Amyloidosis with Initial Manifestations Mimicking Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy
- A Case of Arrhythmogenic Right Ventricular Dysplasia
- Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy: Report of an Autopsy Case
- Arrhythmogenic Noncompaction Cardiomyopathy: Is There an Echocardiographic Phenotypic Overlap of Two Distinct Cardiomyopathies?
- A case of arrhythmogenic right ventricular cardiomyopathy/dysplasia involving the left ventricle
