Ann Rehabil Med.
2016 Feb;40(1):168-171. 10.5535/arm.2016.40.1.168.
Bilateral Cranial IX and X Nerve Palsies After Mild Traumatic Brain Injury
- Affiliations
-
- 1Department of Rehabilitation Medicine, Kyung Hee University, Seoul, Korea. sungjoon.chung@gmail.com
- KMID: 2155180
- DOI: http://doi.org/10.5535/arm.2016.40.1.168
Abstract
- We report a 57-year-old man with bilateral cranial nerve IX and X palsies who presented with severe dysphagia. After a mild head injury, the patient complained of difficult swallowing. Physical examination revealed normal tongue motion and no uvular deviation. Cervical X-ray findings were negative, but a brain computed tomography revealed a skull fracture involving bilateral jugular foramen. Laryngoscopy indicated bilateral vocal cord palsy. In a videofluoroscopic swallowing study, food residue remained in the vallecula and pyriform sinus, and there was reduced motion of the pharynx and larynx. Electromyography confirmed bilateral superior and recurrent laryngeal neuropathy.
MeSH Terms
Figure
-
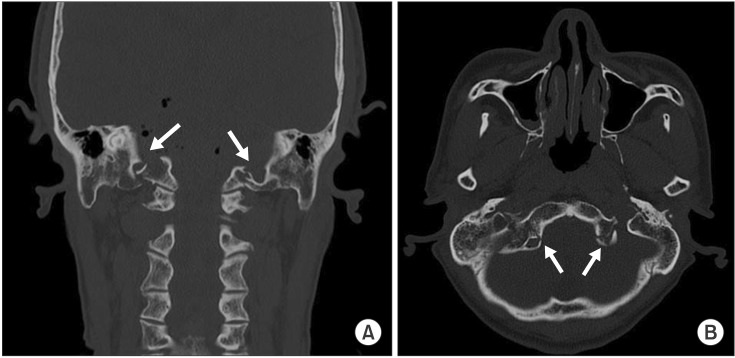
Fig. 1 Transverse (A) and coronal (B) computed tomography revealed bilateral occipital condylar fracture (arrow) extending to the jugular foramina.

Fig. 2 Laryngoscopy showed incomplete movement of bilateral vocal cord.

Fig. 3 The videofluoroscopic swallowing study showed a large amount of vallecular residue due to absence of the swallowing reflex: (A) anteroposterior view and (B) lateral view.
Reference
-
1. Legros B, Fournier P, Chiaroni P, Ritz O, Fusciardi J. Basal fracture of the skull and lower (IX, X, XI, XII) cranial nerves palsy: four case reports including two fractures of the occipital condyle: a literature review. J Trauma. 2000; 48:342–348. PMID: 10697104.2. Lehn AC, Lettieri J, Grimley R. A case of bilateral lower cranial nerve palsies after base of skull trauma with complex management issues: case report and review of the literature. Neurologist. 2012; 18:152–154. PMID: 22549358.3. Sharma BS, Mahajan RK, Bhatia S, Khosla VK. Collet-Sicard syndrome after closed head injury. Clin Neurol Neurosurg. 1994; 96:197–198. PMID: 7924092.
Article4. Tuli S, Tator CH, Fehlings MG, Mackay M. Occipital condyle fractures. Neurosurgery. 1997; 41:368–377. PMID: 9257304.
Article5. Wen HT, Rhoton AL Jr, Katsuta T, de Oliveira E. Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg. 1997; 87:555–585. PMID: 9322846.
Article6. Coello AF, Canals AG, Gonzalez JM, Martin JJ. Cranial nerve injury after minor head trauma. J Neurosurg. 2010; 113:547–555. PMID: 20635856.
Article7. Capuano C, Costagliola C, Shamsaldin M, Maleci A, Di Lorenzo N. Occipital condyle fractures: a hidden nosologic entity. An experience with 10 cases. Acta Neurochir (Wien). 2004; 146:779–784. PMID: 15254800.
Article8. Urculo E, Arrazola M, Arrazola M Jr, Riu I, Moyua A. Delayed glossopharyngeal and vagus nerve paralysis following occipital condyle fracture: case report. J Neurosurg. 1996; 84:522–525. PMID: 8609569.9. Brown H. Anatomy of the spinal accessory nerve plexus: relevance to head and neck cancer and atherosclerosis. Exp Biol Med (Maywood). 2002; 227:570–578. PMID: 12192098.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Associated Injuries and Prognosis in Traumatic Isolated 3rd, 4th, and 6th Cranial Nerve Palsies
- 1 case of relapsed leprosy accompanied by multiple cranial nerve palsies
- Cranial nerve injuries in the adult with traumatic brain injury
- Etiology of Isolated Third, Fourth, and Sixth Cranial Nerve Palsies with a Cancer History
- Type 1 Lissencephaly with Ocular Abnormality and Cranial Nerve Palsies
