Acute Fulminant Myocarditis Recovered from Electro-Mechanical Dissociation in Scrub Typhus
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University Gangnam Severance Hospital, Seoul, Korea. cardiobk@yuhs.ac
- KMID: 2152749
- DOI: http://doi.org/10.12771/emj.2016.39.1.1
Abstract
- Scrub typhus, caused by Orientia tsutsugamushi, is an acute febrile illness. Characteristics of tsutsugamushi disease are fever, rash and eschar. However, severe complications might rarely occur, such as acute fulminant myocarditis caused by scrub typhus. Thus, there are few reports of recovery from seriously complicated cases. We report on an adult male with scrub typhus complicated with acute fulminant myocarditis with no previous comorbid illness who recovered successfully with proper treatment including antibiotics, ventilator support, percutaneous cardiopulmonary support, and continuous renal replacement therapy.
MeSH Terms
Figure
-

Fig. 1 The initial chest X-ray shows increased interstitial markings in both lung fields, mediastinal widening and cardiomegaly.
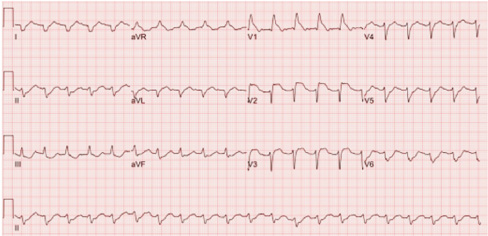
Fig. 2 Electrocardiography on admission shows sinus tachycardia, right bundle branch block, ST depression in lead II, III aVF, and ST elevation in lead V1-3.
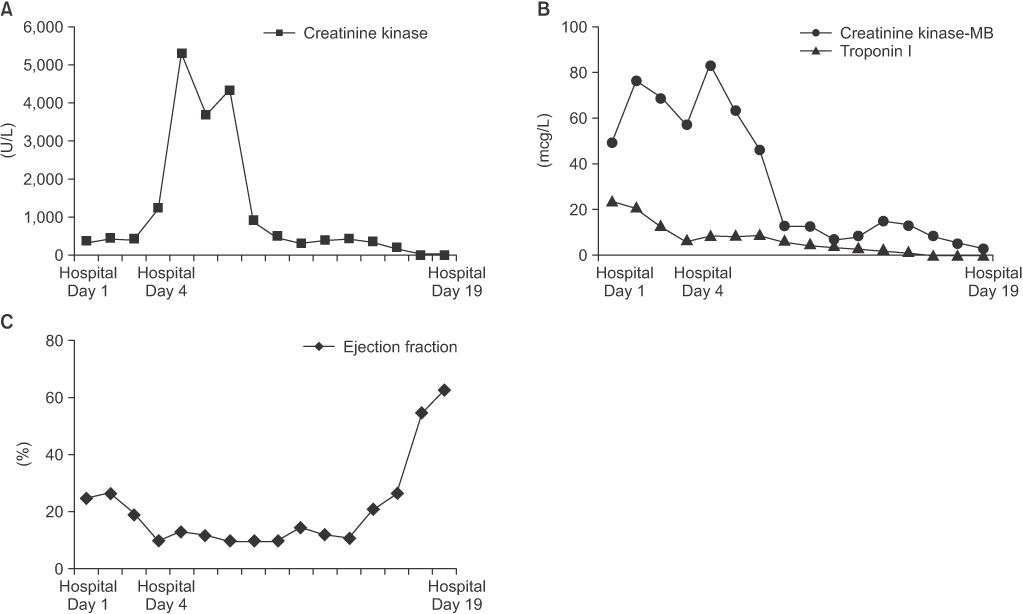
Fig. 3 Changes in cardiac markers―(A) creatinine kinase, (B) creatinine kinase-MB and troponin I―and (C) ejection fraction.
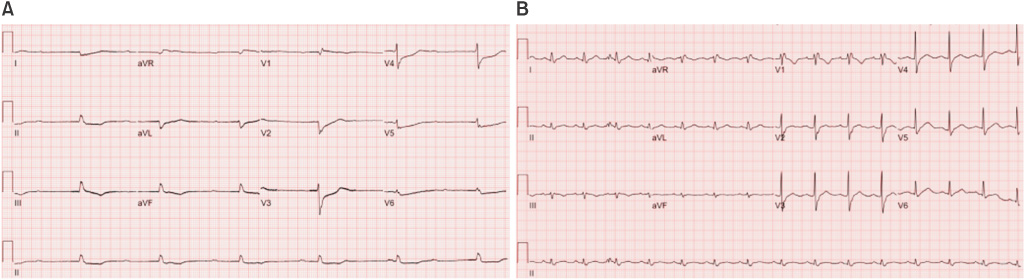
Fig. 4 On the 4th day of hospitalization, electrocardiography shows atrioventricular dissociation (A). After improvement, electrocardiography shows normal atrio-ventricular conduction (B).
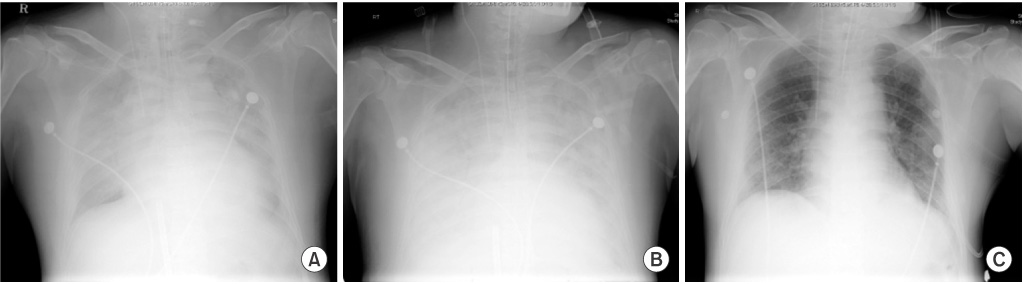
Fig. 5 During the follow up period, chest X-ray shows pleural effusion and pulmonary edema and cardiomegaly, and aggravation for about a week. After three weeks of admission, clinical improvement has been observed and chest X-ray shows improvement of pleural effusion and pulmonary edema and cardiomegaly. On the (A) 4th, (B) 8th, (C) 19th day of hospitalization.
Reference
-
1. Tsay RW, Chang FY. Acute respiratory distress syndrome in scrub typhus. QJM. 2002; 95:126–128.2. Levine HD. Pathologic study of thirty-one cases of scrub typhus fever with especial reference to the cardiovascular system. Am Heart J. 1946; 31:314–328.3. Yotsukura M, Aoki N, Fukuzumi N, Ishikawa K. Review of a case of tsutsugamushi disease showing myocarditis and confirmation of Rickettsia by endomyocardial biopsy. Jpn Circ J. 1991; 55:149–153.4. Han DJ, Park HS, Kim DY, Kang HC, Rhee HS, Lee SW, et al. Acute fulminant myocarditis following scrub typhus infection. Korean J Med. 2013; 85:623–628.5. Jeong YJ, Kim S, Wook YD, Lee JW, Kim KI, Lee SH. Scrub typhus: clinical, pathologic, and imaging findings. Radiographics. 2007; 27:161–172.6. Brown GW, Shirai A, Rogers C, Groves MG. Diagnostic criteria for scrub typhus: probability values for immunofluorescent antibody and Proteus OXK agglutinin titers. Am J Trop Med Hyg. 1983; 32:1101–1107.7. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000; 343:1388–1398.8. Cooper LT Jr. Myocarditis. N Engl J Med. 2009; 360:1526–1538.9. Magnani JW, Dec GW. Myocarditis: current trends in diagnosis and treatment. Circulation. 2006; 113:876–890.10. Sittiwangkul R, Pongprot Y, Silviliarat S, Oberdorfer P, Jittamala P, Sirisanthana V. Acute fulminant myocarditis in scrub typhus. Ann Trop Paediatr. 2008; 28:149–154.11. Park JJ, Cho HJ. Mechanical circulatory support for advanced heart failure. Korean J Med. 2015; 88:142–149.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Fulminant Myocarditis Following Scrub Typhus Infection
- Scrub typhus with complications of acute myocarditis and cardiac tamponade in metropolitan areas: two case reports
- A Case of Scrub Typhus with Acute Respiratory Distress Symdrome and Meningoencephalitis
- Three Cases of Scrub Typhus with Acute Epiglottitis
- A Case of Scrub Typhus with Bilateral Sudden Hearing Loss
