Cross-sectional Study of Patients with Diffuse Large B-Cell Lymphoma: Assessing the Effect of Host Status, Tumor Burden, and Inflammatory Activity on Venous Thromboembolism
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kstwoh@skku.edu
- 2Biostatistics Team, Samsung Biomedical Research Institute, Seoul, Korea.
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2152290
- DOI: http://doi.org/10.4143/crt.2014.266
Abstract
- PURPOSE
The risk factors for venous thromboembolism (VTE) in diffuse large B-cell lymphoma (DLBCL) are not clear although thrombosis can be associated with host status, tumor burden, and inflammatory activity. We assessed the effect of those factors on VTE in a cross-sectional study of patients enrolled in a prospective cohort study.
MATERIALS AND METHODS
We analyzed the occurrence of VTE in 322 patients with newly diagnosed DLBCL who received rituximab with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) between 2008 and 2011. Serum levels of inflammatory cytokines were measured from serum samples archived at diagnosis.
RESULTS
With a median follow-up duration of 41.9 months, VTE was documented in 34 patients (10.6%). A comparison of baseline characteristics indicated the group with VTE had higher percentage of old age, stage III/IV and extranodal involvements than the group without VTE (p < 0.05). Thus, the International Prognostic Index was significantly associated with VTE, but the Khorana score was not. A univariate competing risk factor analysis for VTE revealed that increased levels of inflammatory cytokines such as interleukin (IL)-6 and IL-10 were also associated with VTE (p < 0.05) in addition to host and tumor burden. However, a multivariate analysis showed that two host factors including age (> or = 60 years) and poor performance were independent risk factors for VTE.
CONCLUSION
Among potential risk factors for VTE including tumor burden and inflammatory activity, age and performance status had a strong impact on the occurrence of VTE in patients with DLBCL who received R-CHOP.
MeSH Terms
-
B-Lymphocytes*
Cohort Studies
Cross-Sectional Studies*
Cyclophosphamide
Cytokines
Diagnosis
Doxorubicin
Drug Therapy
Follow-Up Studies
Humans
Interleukin-10
Interleukins
Lymphoma, B-Cell*
Multivariate Analysis
Prednisone
Prospective Studies
Risk Factors
Thrombosis
Tumor Burden*
Venous Thromboembolism*
Vincristine
Cyclophosphamide
Cytokines
Doxorubicin
Interleukin-10
Interleukins
Prednisone
Vincristine
Figure
-

Fig. 1. Study design: cross-sectional analysis. This prospective cohort study aimed to develop a predictive model for treatment outcomes and treatment-related morbidity (such as VTE in this study) in patients with lymphoma. VTE, venous thromboembolism; DLBCL, diffuse large B-cell lymphoma; LDH, lactate dehydrogenase; IPI, International Prognostic Index; CRP, C-reactive protein.
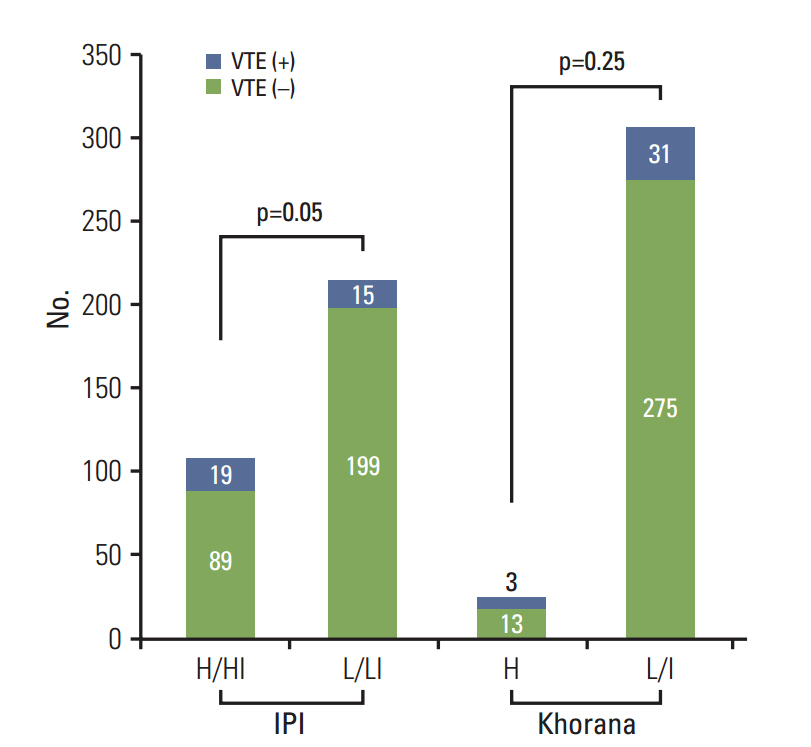
Fig. 2. Comparison of International Prognostic Index (IPI) and Khorana score on the occurrence of venous thromboembolism (VTE). Patients with high or high-intermediate (H/HI) IPI risk (18%, 19/108) had significantly more VTE events than those with low or low-intermediate (L/LI) IPI risk (7%, 15/214; p=0.05). Khorana risk classification did not show significant association with VTE (Khorana score high [≥ 3] group [H], 24%; low/intermediate group [L/I], 10%; p=0.25).
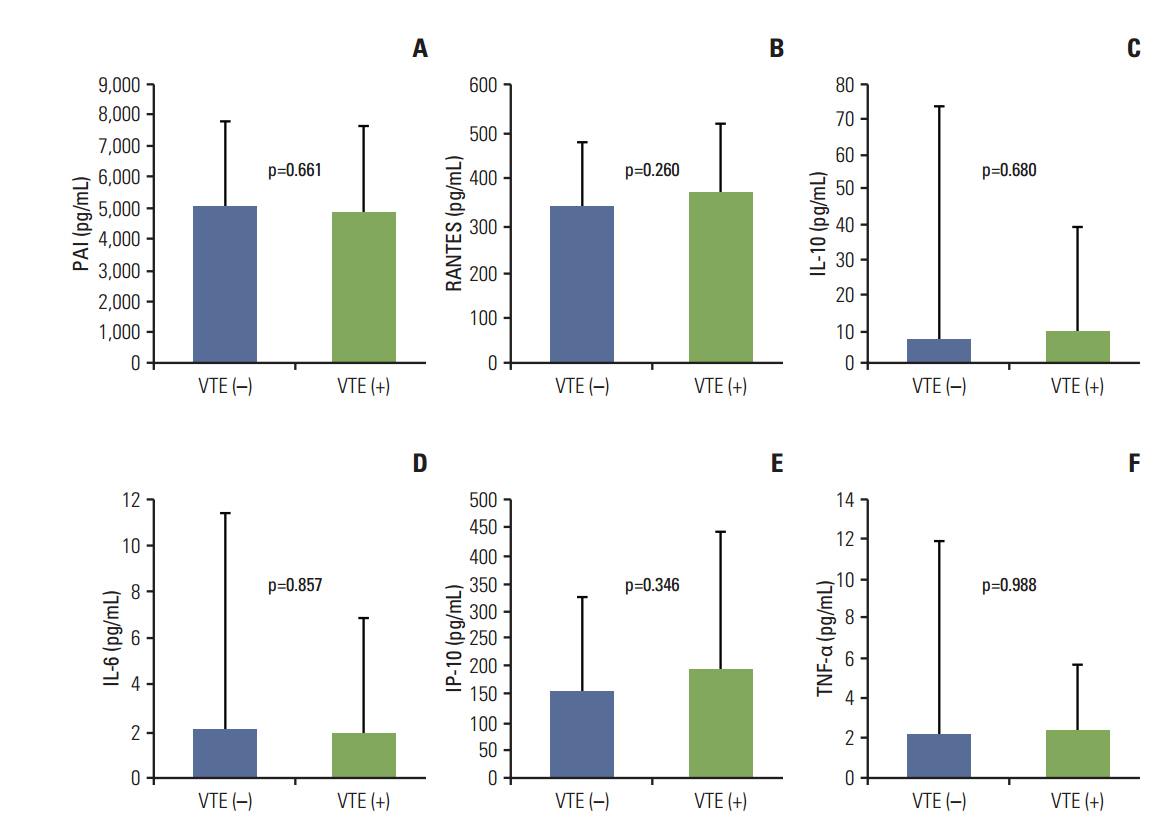
Fig. 3. Comparison of inflammatory biomarkers in patients with and without venous thromboembolism (VTE). The mean serum levels of inflammatory biomarkers plasminogen activator inhibitor-1 (PAI) (A), regulated on activation, normal T cell expressed and secreted (RANTES) (B), interleukin (IL) 10 (C), IL-6 (D), interferon gamma-induced protein 10 (IP-10) (E), and tumor necrosis factor α (TNF-α) (F) were not significantly different between patients with and without VTE.
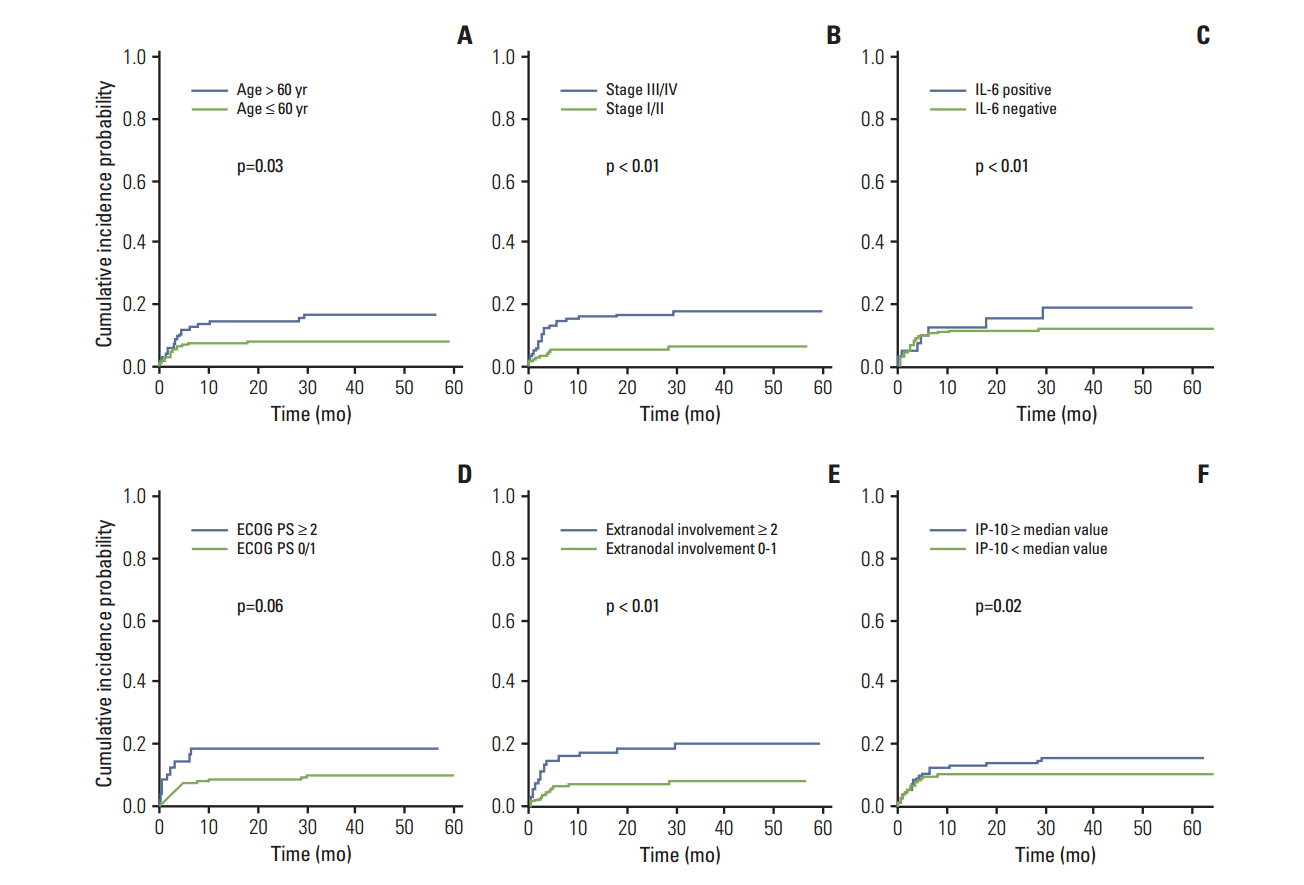
Fig. 4. Comparison of host factors, tumor burden and inflammatory cytokines on the occurrence of venous thromboembolism (VTE). The occurrence of VTE was associated with old age (A), advanced stage (B), presence of interleukin (IL) 6 (C), poor PS (D), extranodal involvements (E), and elevated serum interferon gamma-induced protein 10 (IP-10) level (F). ECOG PS, Eastern Cooperative Oncology Group performance status.

Fig. 5. Comparison of survival rates between patients with and without venous thromboembolism (VTE). The overall survival rate was not significantly different between patients with or without VTE.
Reference
-
References
1. Lekovic D, Miljic P, Mihaljevic B. Increased risk of venous thromboembolism in patients with primary mediastinal large B-cell lymphoma. Thromb Res. 2010; 126:477–80.
Article2. Caruso V, Di Castelnuovo A, Meschengieser S, Lazzari MA, de Gaetano G, Storti S, et al. Thrombotic complications in adult patients with lymphoma: a meta-analysis of 29 independent cohorts including 18 018 patients and 1149 events. Blood. 2010; 115:5322–8.
Article3. Huh J. Epidemiologic overview of malignant lymphoma. Korean J Hematol. 2012; 47:92–104.
Article4. Coiffier B. State-of-the-art therapeutics: diffuse large B-cell lymphoma. J Clin Oncol. 2005; 23:6387–93.
Article5. Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002; 346:235–42.
Article6. Coiffier B, Thieblemont C, Van Den Neste E, Lepeu G, Plantier I, Castaigne S, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d'Etudes des Lymphomes de l'Adulte. Blood. 2010; 116:2040–5.
Article7. Yokoyama K, Murata M, Ikeda Y, Okamoto S. Incidence and risk factors for developing venous thromboembolism in Japanese with diffuse large b-cell lymphoma. Thromb Res. 2012; 130:7–11.
Article8. Park LC, Woo SY, Kim S, Jeon H, Ko YH, Kim SJ, et al. Incidence, risk factors and clinical features of venous thromboembolism in newly diagnosed lymphoma patients: results from a prospective cohort study with Asian population. Thromb Res. 2012; 130:e6.
Article9. Ferroni P, Riondino S, Formica V, Cereda V, Tosetto L, La Farina F, et al. Venous thromboembolism risk prediction in ambulatory cancer patients: clinical significance of neutrophil/lymphocyte ratio and platelet/lymphocyte ratio. Int J Cancer. 2015; 136:1234–40.
Article10. Prandoni P, Falanga A, Piccioli A. Cancer and venous thromboembolism. Lancet Oncol. 2005; 6:401–10.
Article11. Reitsma PH, Rosendaal FR. Activation of innate immunity in patients with venous thrombosis: the Leiden Thrombophilia Study. J Thromb Haemost. 2004; 2:619–22.
Article12. Mause SF, von Hundelshausen P, Zernecke A, Koenen RR, Weber C. Platelet microparticles: a transcellular delivery system for RANTES promoting monocyte recruitment on endothelium. Arterioscler Thromb Vasc Biol. 2005; 25:1512–8.13. Lv W, Duan Q, Wang L, Gong Z, Yang F, Song Y. Gene expression levels of cytokines in peripheral blood mononuclear cells from patients with pulmonary embolism. Mol Med Rep. 2013; 7:1245–50.
Article14. Komrokji RS, Uppal NP, Khorana AA, Lyman GH, Kaplan KL, Fisher RI, et al. Venous thromboembolism in patients with diffuse large B-cell lymphoma. Leuk Lymphoma. 2006; 47:1029–33.
Article15. Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007; 110:2339–46.
Article16. Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008; 111:4902–7.
Article17. Khorana AA, Francis CW, Culakova E, Lyman GH. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer. 2005; 104:2822–9.
Article18. Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996; 17:343–6.
Article19. Ay C, Dunkler D, Marosi C, Chiriac AL, Vormittag R, Simanek R, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010; 116:5377–82.
Article20. Fox EA, Kahn SR. The relationship between inflammation and venous thrombosis: a systematic review of clinical studies. Thromb Haemost. 2005; 94:362–5.
Article21. van Aken BE, den Heijer M, Bos GM, van Deventer SJ, Reitsma PH. Recurrent venous thrombosis and markers of inflammation. Thromb Haemost. 2000; 83:536–9.
Article22. Poredos P, Jezovnik MK. In patients with idiopathic venous thrombosis, interleukin-10 is decreased and related to endothelial dysfunction. Heart Vessels. 2011; 26:596–602.
Article23. Christiansen SC, Naess IA, Cannegieter SC, Hammerstrom J, Rosendaal FR, Reitsma PH. Inflammatory cytokines as risk factors for a first venous thrombosis: a prospective population-based study. PLoS Med. 2006; 3:e334.
Article24. Incalcaterra E, Meli F, Muratori I, Corrado E, Amato C, Canino B, et al. Residual vein thrombosis and onset of post-thrombotic syndrome: influence of the 4G/5G polymorphism of plasminogen activator inhibitor-1 gene. Thromb Res. 2014; 133:371–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relapse of Ocular Lymphoma following Primary Testicular Diffuse Large B-cell Lymphoma
- A Case of Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma Occurring in Thyroid Gland
- The Expression of p16 in Diffuse Large B-cell Lymphoma and Its Prognostic Implications
- Inverse Psoriasis Developed in a Patient with Diffuse Large B Cell Lymphoma
- Relationships among Hepatitis C Virus, Hepatocellular Carcinoma, and Diffuse Large B Cell Lymphoma: A Case Report
