Prog Med Phys.
2015 Dec;26(4):267-272. 10.14316/pmp.2015.26.4.267.
The Dose and Risk Reduction from Adoption of Automatic mA Control in 4D CT Scans
- Affiliations
-
- 1Department of Radiation Oncology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 2Department of Neurosurgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. michael@uuh.ulsan.kr
- KMID: 2151761
- DOI: http://doi.org/10.14316/pmp.2015.26.4.267
Abstract
- In this study, the reduction of dose and risk was evaluated from using automatic mA control in 4D CT scan of patients whose organ movement was considered for gated radiotherapy. The organ doses, CTDI, effective doses from 4D CT with and without using automatic mA control were evaluated using CT-Expo program for each 10 patients of liver and lung cancer, and the risk of exposure induced death and loss of life expectancy were evaluated using PCXMC program. It was founded that there were 26.8%, and 15.5% dose reduction in organ doses and CTDI for liver and lung cancer patients and 16.5% and 19.8% risk reduction in liver and lung cancer patients. The organ doses and effective doses were evaluated for the parameter of each patient used in CT scans, and risks considering age and gender could be evaluated. It was founded that there were 21.2% dose reduction and 18.2% risk reduction in 4D CT scan using AEC for liver and lung cancer patients.
Keyword
MeSH Terms
Figure
-
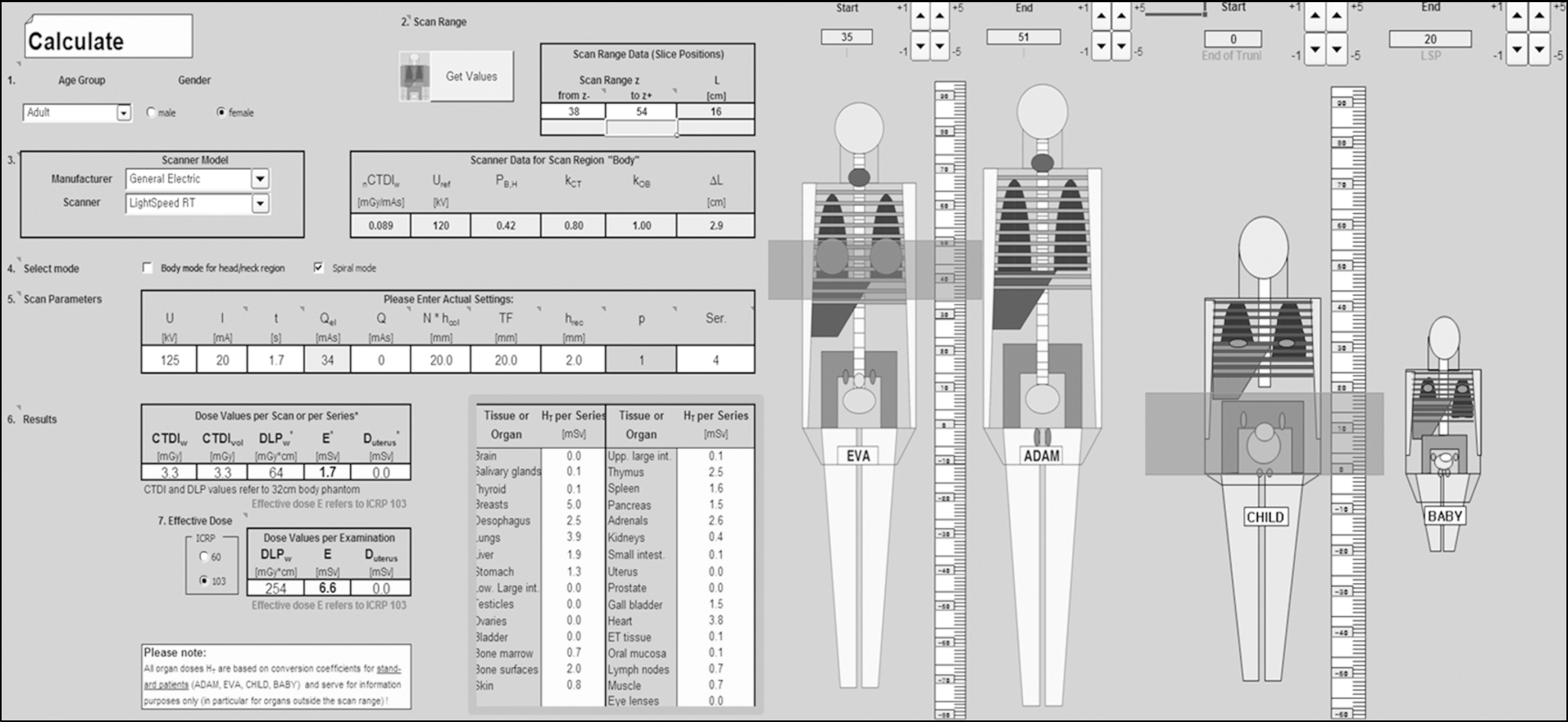
Fig. 1. Screen shot of CT-Expo.
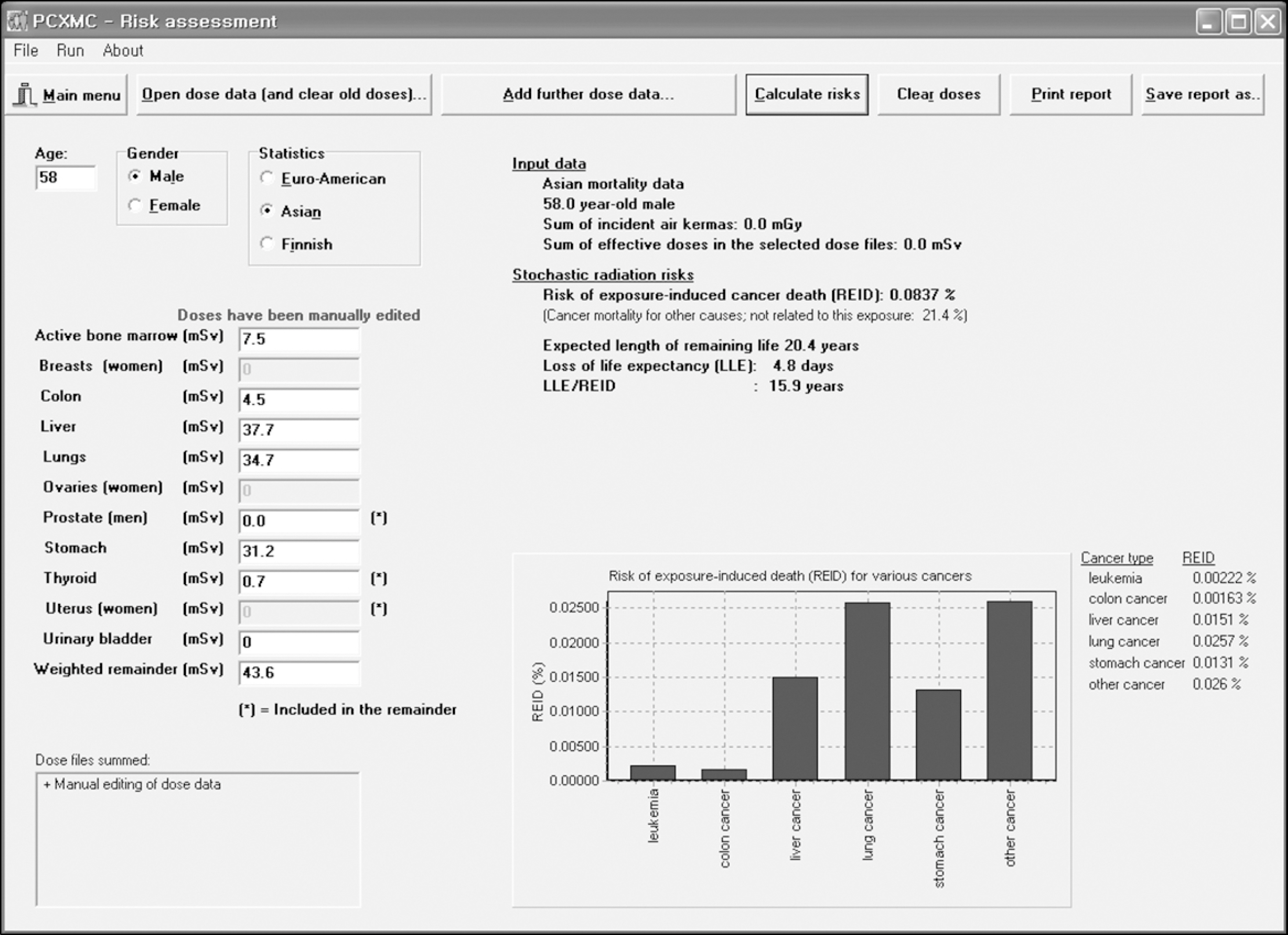
Fig. 2. Screen shot risk assessment module of PCXMC.
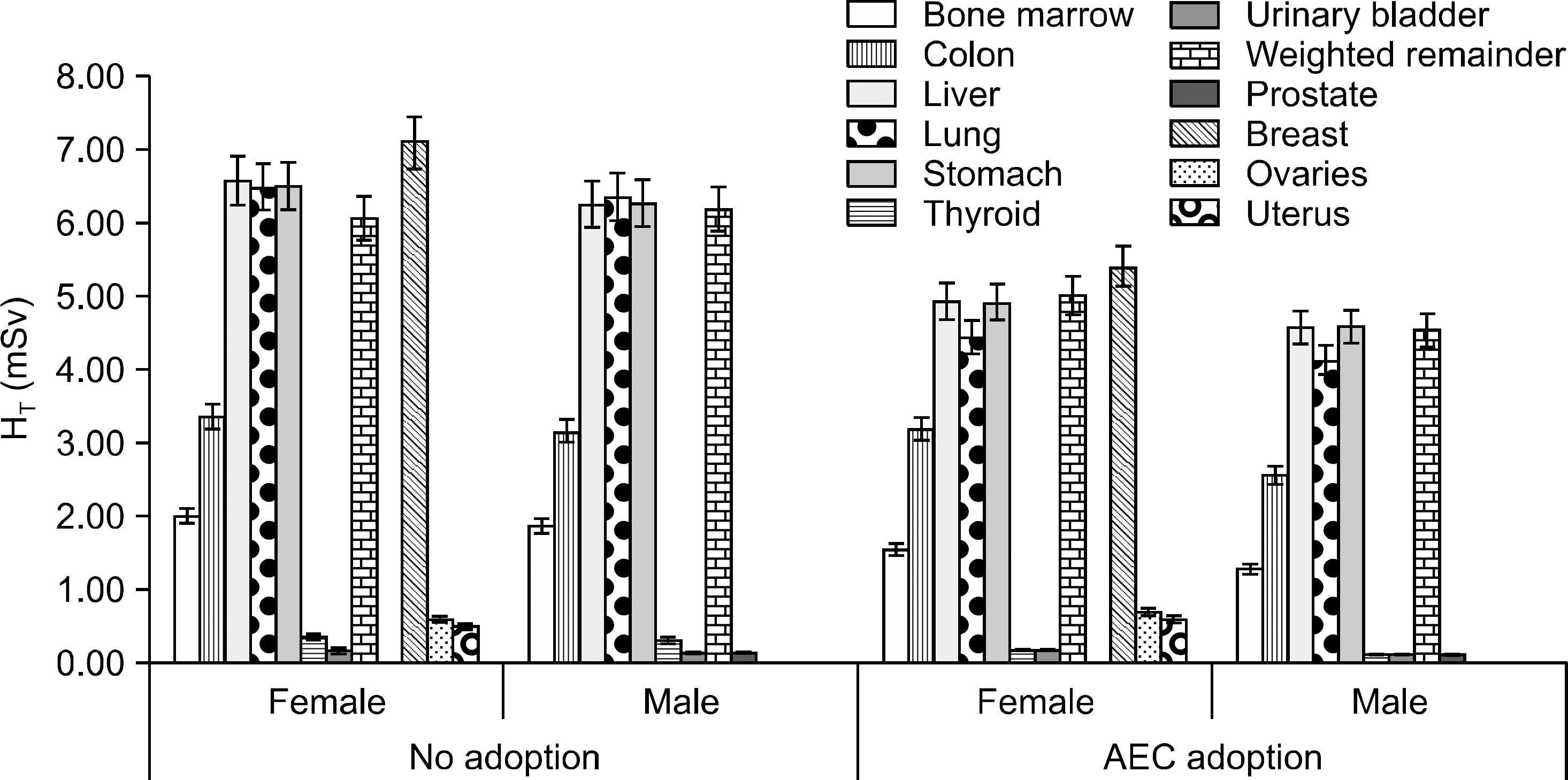
Fig. 3. Calculated organ doses from 4D CT scan for Liver cancer patients.

Fig. 4. Calculated organ doses from 4D CT scan for Lung cancer patients.
Reference
-
References
1. Mettler FA, Jr. , Bhargavan M, Faulkner K, et al. Radiologic and nuclear medicine studies in the United States and worldwide: frequency, radiation dose, and comparison with other radiation sources–1950–2007. Radiology. 253(2):520–531. 2009.
Article2. Measurements NCoRPa: Ionizing Radiation Exposure of the Population of the United States. Report No. 160 (. 2009.3. Stamm G, Nagel HD. [CT-expo–a novel program for dose evaluation in CT]. Rofo. 174(12):1570–1576. 2002.4. ICRP: 1990 Recommendations of the International Commission on Radiological Protection. ICRP Publication 60. Ann. ICRP 21 (1–3) (. 1991.5. ICRP: The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37 (2–4). (. 2007.6. Tapiovaara M S. PCXMC –A Monte Carlo program for calculating patient doses in medical x-ray examinations (2nd Ed.). STUK-A 231 (STUK-A 231) (2008.).7. Council NR. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2 (. 2006.8. Thomas D, Darby S, Fagnani F, Hubert P, Vaeth M, Weiss K. Definition and estimation of lifetime detriment from radiation exposures: principles and methods. Health Phys. 63(3):259–272. 1992.9. McCollough CH, Bruesewitz MR, Kofler JM, Jr.: CT dose reduction and dose management tools: overview of available options. Radiographics. 26(2):503–512. 2006.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dosimetric Effects of Low Dose 4D CT Using a Commercial Iterative Reconstruction on Dose Calculation in Radiation Treatment Planning: A Phantom Study
- CT radiation dose and radiation reduction strategies
- Four-Dimensional Thoracic CT in Free-Breathing Children
- In-Plane Shielding for CT: Effect of Off-Centering, Automatic Exposure Control and Shield-to-Surface Distance
- Estimation of Radiation Exposure of 128-Slice 4D-Perfusion CT for the Assessment of Tumor Vascularity
