Use of an Ultrasonic Osteotome for Direct Removal of Beak-Type Ossification of Posterior Longitudinal Ligament in the Thoracic Spine
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea. chungc@snu.ac.kr
- 2Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea.
- 3Clinical Research Institute, Seoul National University Hospital, Seoul, Korea.
- 4Department of Orthopedic Surgery, Orthopaedic Associates of Dutchess County/Vassar Brothers Medical Center, Poughkeepsie, NY, USA.
- 5Department of Brain and Cognitive Sciences, Seoul National University College of Natural Sciences, Seoul, Korea.
- KMID: 2151164
- DOI: http://doi.org/10.3340/jkns.2015.58.6.571
Abstract
- Direct removal of beak-type ossification of posterior longitudinal ligament at thoracic spine (T-OPLL) is a challenging surgical technique due to the potential risk of neural injury. Slipping off the cutting surface of a high-speed drill may result in entrapment in neural structures, leading to serious complications. Removal of T-OPLL with an ultrasonic osteotome, utilizing back and forth micro-motion of a blade rather than rotatory-motion of drill, may reduce such complications. We have applied the ultrasonic osteotome for posterior circumferential decompression of T-OPLL for three consecutive patients with beak-type OPLL and have described the surgical techniques and patient outcomes. The preoperative chief complaint was gait disturbance in all patients. Japanese orthopedic association scores (JOA) was used for functional assessment. Scores measured 2/11, 5/11, 2/11, and 4/11 for each patient. The ventral T-OPLL mass was exposed after posterior midline approach, laminotomy and transeversectomy. The T-OPLL mass was directly removed with an ultrasonic osteotome and instrumented segmental fixation was performed. The surgeries were uneventful. Detailed surgical techniques were presented. Gait disturbance was improved in all patients. Dural tear occurred in one patient without squeal. Postoperative JOA was 6/11, 10/11, 8/11, and 8/11 (recovery rate; 44%, 83%, 67%, and 43%) respectively at 18, 18, 10, and 1 months postoperative. T-OPLL was completely removed in all patients as confirmed with computed tomography scan. We hope that surgical difficulties in direct removal of T-OPLL might be reduced by utilizing ultrasonic osteotome.
Keyword
MeSH Terms
Figure
-

Fig. 1 Ultrasonic osteotome. Various kinds of tips could be attached to the hand piece according to the purpose of surgery (A). The blade (B, left) was used for laminotomy and shaving tips (B, middle and right) were preferentially used in direct removal of ossified mass.
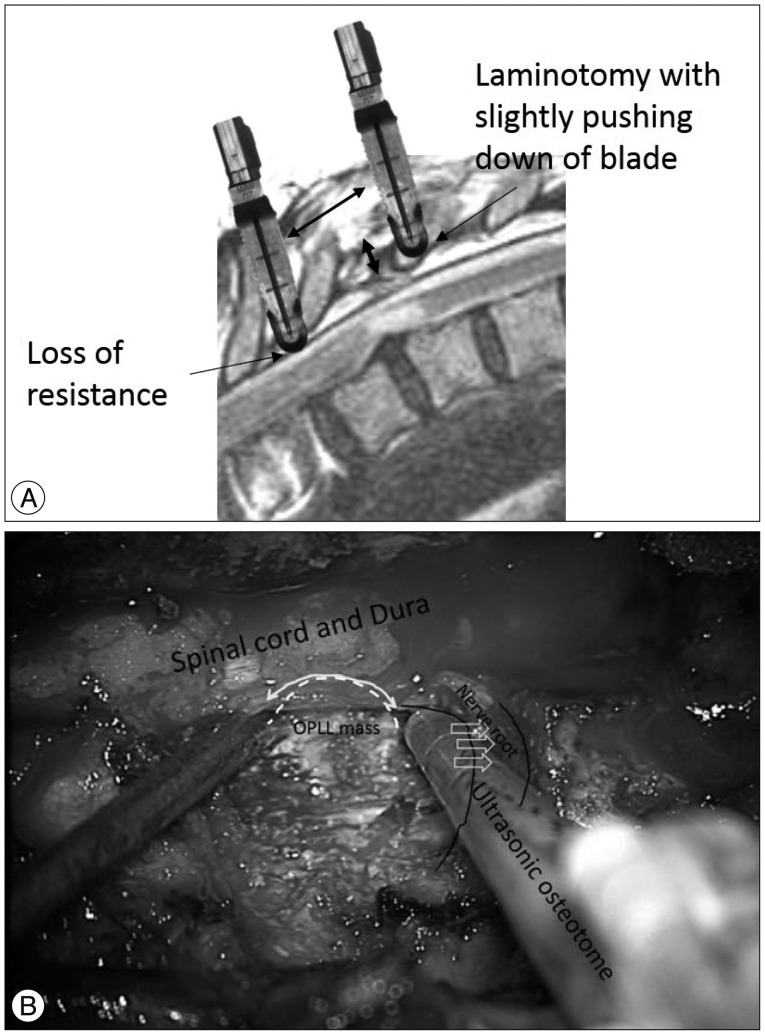
Fig. 2 A : The lamina was gradually cut with ultrasonic osteotome by slight pushing down its blade against lamina with a vertical motion (right blade). When inner cortical bone was cut, loss of resistance was felt (left blade) and the ostetome was not inserted beyond the depth. Then the ostetome was moved cranially and caudally along the lamina for laminotomy. B : After laminotomy, facetectomy and pediclectomy, ossification of posterior longitudinal ligament (OPLL) mass was exposed under the dura (white broken line). The ultrasonic osteotome was inserted at the base of OPLL mass and moved gradually along the OPLL mass (white curved arrow). Note that nerve root was retracted with the shaft of ultrasonic osteotome. Because the energy was not transmitted from the shaft, the osteotome could be inserted at the base of OPLL mass while retracting nerve root.

Fig. 3 Case 3. Sagittal magnetic resonance (MR) T2-weighted imaging (A), sagittally reconstructed (B), axial (C) and 3-D (D) computed tomography (CT) scan showed beak-type ossified posterior longitudinal ligament (OPLL). The level of the axial scan was marked in sagittal CT scan with a black line. Postoperative sagittally reconstructed CT scan (E) showed complete removal of OPLL mass (F, white line in E), but a small fragment was left at T7 (G, arrow, black line in E). A 3-D reconstructed CT scan showed instrumentation, removal of OPLL (H, arrow) and laminoplasty with miniplate (I).
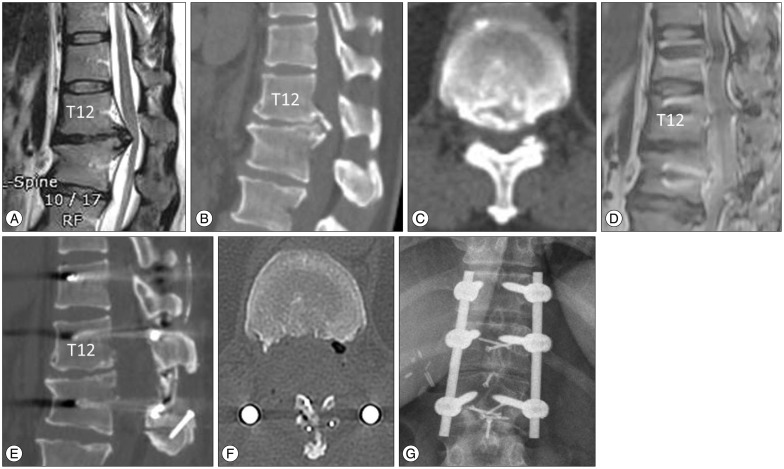
Fig. 4 Case 4. Sagittal magnetic resonance (MR) T2-weighted imaging (A), sagittally reconstructed (B), and axial (C) computed tomography (CT) scan showed beak-type ossified posterior longitudinal ligament (OPLL). Postoperative sagittal MR imaging (D) and sagittal (E) and axial CT scans (F) showed complete removal of T-OPLL mass. The laminoplasty was performed with translaminar screws (G).
Cited by 1 articles
-
Surgical Outcomes According to Dekyphosis in Patients with Ossification of the Posterior Longitudinal Ligament in the Thoracic Spine
Soo Yeon Kim, Seung-Jae Hyun, Ki-Jeong Kim, Tae-Ahn Jahng
J Korean Neurosurg Soc. 2020;63(1):89-98. doi: 10.3340/jkns.2018.0177.
Reference
-
1. Bolesta MJ, Caron T, Chinthakunta SR, Vazifeh PN, Khalil S. Pedicle screw instrumentation of thoracolumbar burst fractures : biomechanical evaluation of screw configuration with pedicle screws at the level of the fracture. Int J Spine Surg. 2012; 6:200–205. PMID: 25694892.
Article2. Chaichana KL, Jallo GI, Dorafshar AH, Ahn ES. Novel use of an ultrasonic bone-cutting device for endoscopic-assisted craniosynostosis surgery. Childs Nerv Syst. 2013; [Epub ahead of print].
Article3. Epstein NE. Medicolegal corner : when minimally invasive thoracic surgery leads to paraplegia. Surg Neurol Int. 2014; 5(Suppl 3):S55–S58. PMID: 24843811.4. Fujimura Y, Nishi Y, Nakamura M, Toyama Y, Suzuki N. Long-term follow-up study of anterior decompression and fusion for thoracic myelopathy resulting from ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 1997; 22:305–311. PMID: 9051893.
Article5. Hanai K, Ogikubo O, Miyashita T. Anterior decompression for myelopathy resulting from thoracic ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 2002; 27:1070–1076. PMID: 12004174.
Article6. Hosono N, Sakaura H, Mukai Y, Ishii T, Yoshikawa H. En bloc laminoplasty without dissection of paraspinal muscles. J Neurosurg Spine. 2005; 3:29–33. PMID: 16122019.
Article7. Hu X, Ohnmeiss DD, Lieberman IH. Use of an ultrasonic osteotome device in spine surgery : experience from the first 128 patients. Eur Spine J. 2013; 22:2845–2849. PMID: 23584231.
Article8. Kawahara N, Tomita K, Murakami H, Hato T, Demura S, Sekino Y, et al. Circumspinal decompression with dekyphosis stabilization for thoracic myelopathy due to ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976). 2008; 33:39–46. PMID: 18165747.
Article9. Kimura H, Fujibayashi S, Takemoto M, Otsuki B, Matsuda S. Spontaneous reduction in ossification of the posterior longitudinal ligament of the thoracic spine after posterior spinal fusion without decompression : a case report. Spine (Phila Pa 1976). 2014; 39:E417–E419. PMID: 24384668.10. Lee SE, Jahng TA, Chung CK, Kim HJ. Circumferential spinal cord decompression through a posterior midline approach with lateral auxiliary ports for lower thoracic compressive myelopathy. Neurosurgery. 2012; 70(2 Suppl Operative):221–229. PMID: 21937940.
Article11. Liu X, Zhu B, Liu X, Liu Z, Dang G. Circumferential decompression via the posterior approach for the surgical treatment of multilevel thoracic ossification of the posterior longitudinal ligaments : a single institution comparative study. Chin Med J (Engl). 2014; 127:3371–3377. PMID: 25269897.12. Ma X, An HS, Zhang Y, Brown NM, Chen Z, Zhang G, et al. A radical procedure of circumferential spinal cord decompression through a modified posterior approach for thoracic myelopathy caused by severely impinging anterior ossification. Spine J. 2014; 14:651–658. PMID: 24161362.
Article13. Matsumoto M, Chiba K, Toyama Y, Takeshita K, Seichi A, Nakamura K, et al. Surgical results and related factors for ossification of posterior longitudinal ligament of the thoracic spine : a multi-institutional retrospective study. Spine (Phila Pa 1976). 2008; 33:1034–1041. PMID: 18427326.
Article14. Matsumoto M, Toyama Y, Chikuda H, Takeshita K, Kato T, Shindo S, et al. Outcomes of fusion surgery for ossification of the posterior longitudinal ligament of the thoracic spine : a multicenter retrospective survey : clinical article. J Neurosurg Spine. 2011; 15:380–385. PMID: 21740130.
Article15. Matsuyama Y, Sakai Y, Katayama Y, Imagama S, Ito Z, Wakao N, et al. Indirect posterior decompression with corrective fusion for ossification of the posterior longitudinal ligament of the thoracic spine : is it possible to predict the surgical results? Eur Spine J. 2009; 18:943–948. PMID: 19347374.
Article16. Matsuyama Y, Yoshihara H, Tsuji T, Sakai Y, Yukawa Y, Nakamura H, et al. Surgical outcome of ossification of the posterior longitudinal ligament (OPLL) of the thoracic spine : implication of the type of ossification and surgical options. J Spinal Disord Tech. 2005; 18:492–497. discussion 498PMID: 16306836.
Article17. McClendon J Jr, Sugrue PA, Ganju A, Koski TR, Liu JC. Management of ossification of the posterior longitudinal ligament of the thoracic spine. Neurosurg Focus. 2011; 30:E16. PMID: 21361754.
Article18. Min JH, Jang JS, Lee SH. Clinical results of ossification of the posterior longitudinal ligament (OPLL) of the thoracic spine treated by anterior decompression. J Spinal Disord Tech. 2008; 21:116–119. PMID: 18391716.
Article19. Miyashita T, Ataka H, Tanno T. Spontaneous reduction of a floated ossification of the ligamentum flavum after posterior thoracic decompression (floating method); report of a case (abridged translation of a primary publication). Spine J. 2013; 13:e7–e9. PMID: 23490728.
Article20. Nickele C, Hanna A, Baskaya MK. Osteotomy for laminoplasty without soft tissue penetration, performed using a harmonic bone scalpel : instrumentation and technique. J Neurol Surg A Cent Eur Neurosurg. 2013; 74:183–186. PMID: 23504672.
Article21. Onishi E, Sano H, Matsushita M. Surgical treatment for thoracic myelopathy due to simultaneous ossification of the posterior longitudinal ligament and ligamentum flavum at the same level. J Spinal Disord Tech. 2013; [Epub ahead of print].
Article22. Park SB, Jahng TA, Kim CH, Chung CK. Thoracic and lumbar laminoplasty using a translaminar screw : morphometric study and technique. J Neurosurg Spine. 2009; 10:603–609. PMID: 19558295.
Article23. Sanborn MR, Balzer J, Gerszten PC, Karausky P, Cheng BC, Welch WC. Safety and efficacy of a novel ultrasonic osteotome device in an ovine model. J Clin Neurosci. 2011; 18:1528–1533. PMID: 21917459.
Article24. Schaeren S, Jaquiéry C, Heberer M, Tolnay M, Vercellotti T, Martin I. Assessment of nerve damage using a novel ultrasonic device for bone cutting. J Oral Maxillofac Surg. 2008; 66:593–596. PMID: 18280402.
Article25. Sugita S, Chikuda H, Takeshita K, Seichi A, Tanaka S. Progression of ossification of the posterior longitudinal ligament of the thoracic spine following posterior decompression and stabilization. J Neurosurg Spine. 2014; 21:773–777. PMID: 25127433.
Article26. Takahata M, Ito M, Abumi K, Kotani Y, Sudo H, Minami A. Clinical results and complications of circumferential spinal cord decompression through a single posterior approach for thoracic myelopathy caused by ossification of posterior longitudinal ligament. Spine (Phila Pa 1976). 2008; 33:1199–1208. PMID: 18469693.
Article27. Tomita K, Kawahara N, Baba H, Kikuchi Y, Nishimura H. Circumspinal decompression for thoracic myelopathy due to combined ossification of the posterior longitudinal ligament and ligamentum flavum. Spine (Phila Pa 1976). 1990; 15:1114–1120. PMID: 2125147.
Article28. Yamazaki M, Mochizuki M, Ikeda Y, Sodeyama T, Okawa A, Koda M, et al. Clinical results of surgery for thoracic myelopathy caused by ossification of the posterior longitudinal ligament : operative indication of posterior decompression with instrumented fusion. Spine (Phila Pa 1976). 2006; 31:1452–1460. PMID: 16741454.
Article29. Yang SH, Kim CH, Chung CK, Park SB, Sohn S, Lee S. Bone fusion rate in the thoracic and lumbar spine after laminoplasty with laminar screws. Spine (Phila Pa 1976). 2014; 39:E1325–E1330. PMID: 25188592.
Article30. Zhang HQ, Chen LQ, Liu SH, Zhao D, Guo CF. Posterior decompression with kyphosis correction for thoracic myelopathy due to ossification of the ligamentum flavum and ossification of the posterior longitudinal ligament at the same level. J Neurosurg Spine. 2010; 13:116–122. PMID: 20594026.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ossification of the Posterior Longitudinal Ligament: 2 cases report
- Circumferential Spinal Cord Decompression through a Single Posterior Approach with Microendoscopy for Thoracic and Thoracolumbar Ossification of the Posterior Longitudinal Ligament
- Ossification of Posterior Longitudinal Ligament
- Ossification of posterior longitudinal ligament of the cervical spine in Korean
- Anterior Decompression and Interbody Fusion for Ossification of the Posterior Longitudinal Ligament of the Cervical Spine: Case Report
