J Korean Ophthalmol Soc.
2015 Jul;56(7):1081-1088. 10.3341/jkos.2015.56.7.1081.
Incidence of Steroid-Induced Ocular Hypertension Following Myopic Refractive Surgery
- Affiliations
-
- 1The Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. kcyeye@yuhs.ac
- 2Eyereum Eye Clinic, Seoul, Korea.
- KMID: 2148809
- DOI: http://doi.org/10.3341/jkos.2015.56.7.1081
Abstract
- PURPOSE
To determine the incidence of steroid-induced ocular hypertension following myopic vision correction.
METHODS
This study retrospectively reviewed the medical records of 6,087 patients (12,164 eyes) who underwent myopic refractive surgery (laser-assisted in-situ keratomileusis [LASIK]/photorefractive keratectomy [PRK]/phakic intraocular lens [IOL] implantation) at Eyereum Eye Clinic between July 2011 and February 2013. Ocular hypertension was defined when post-operative intraocular pressure (IOP) was increased more than 30% compared to predicted IOP adjusted according to corneal thickness. All preoperative IOPs were measured using Goldmann applanation tonometer (GAT). Postoperative IOPs were measured using non-contact tonometer first and with GAT when the IOP was suspiciously increased.
RESULTS
Steroid-induced ocular hypertension after a myopic refractive surgery occurred in 680 eyes (5.58%) of 404 patients (6.64%). The incidence based on surgery was LASIK (0.06%, 2/3, 514 eyes) followed by PRK (7.63%, 575/7,533 eyes) and phakic IOL implantation (9.2%, 103/1,117 eyes). The average increased IOP level in patients with steroid-induced ocular hypertension was 5.62 +/- 3.73 mm Hg after PRK and 9.35 +/- 4.95 mm Hg after phakic IOL implantation. A statistically significantly higher change in IOP was observed in the phakic IOL group (p < 0.001). However, the PRK group had a longer treatment period for ocular hypertension and used more antiglaucoma medications than the phakic IOL group (p < 0.05). Most patients with ocular hypertension were successfully treated with cessation of topical steroid or use of antiglaucoma medications. Only 2 eyes required glaucoma surgery because IOP was not controlled.
CONCLUSIONS
IOP measurements should be initiated no later than 1 week after surgery because steroid-induced ocular hypertension following myopic refractive surgery can occur in approximately 5.58% of patients and most cases of ocular hypertension can be controlled with careful follow-up and use of antiglaucoma medications.
MeSH Terms
Figure
-

Figure 1. Management of the steroid induced ocular hyper-tension after myopic refractive surgery. IOP = intraocular pressure.
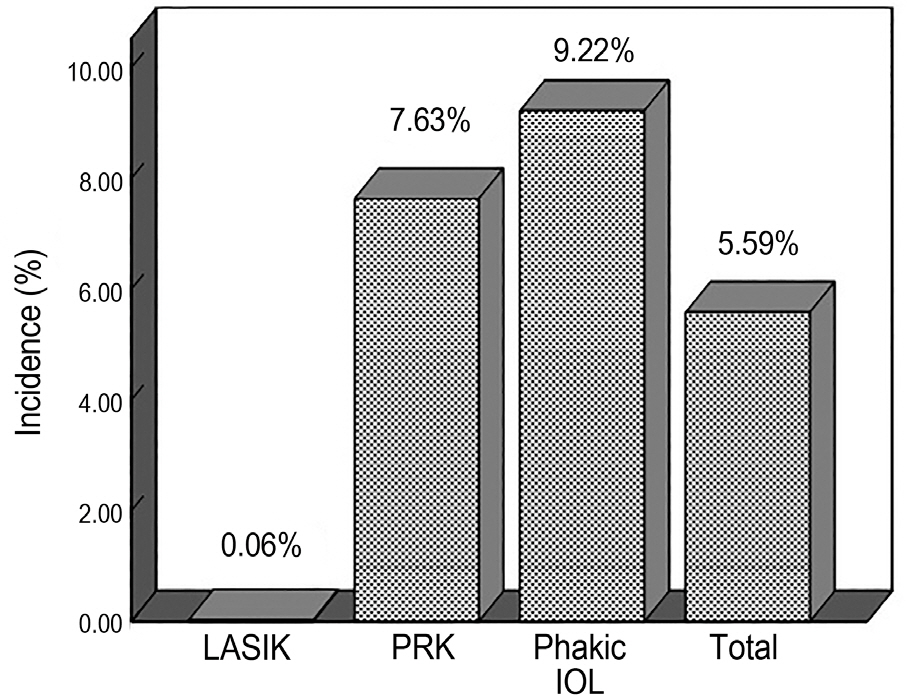
Figure 2. The incidence of the steroid-induced ocular hypertension in each group after myopic refractive surgery between July 2011 and February 2013. LASIK = laser-assisted in-situ keratomileusis; PRK = photorefractive keratectomy; IOL = intraocular lens.
Reference
-
References
1. Smith RJ, Maloney RK. Diffuse lamellar keratitis. A new syn-drome in lamellar refractive surgery. Ophthalmology. 1998; 105:1721–6.
Article2. Peters NT, Lingua RW, Kim CH. Topical intrastromal steroid dur-ing laser in situ keratomileusis to retard interface keratitis. J Cataract Refract Surg. 1999; 25:1437–40.
Article3. Nagy ZZ, Szabó A, Krueger RR, Süveges I. Treatment of intra-ocular pressure elevation after photorefractive keratectomy. J Cataract Refract Surg. 2001; 27:1018–24.
Article4. Tengroth B, Epstein D, Fagerholm P, et al. Excimer laser photo-refractive keratectomy for myopia: clinical results in sighted eyes. Ophthalmology. 1993; 100:739–45.5. McPherson R, Hanna K, Agro A, et al. Cerivastatin versus branded pravastatin in the treatment of primary hypercholesterolemia in primary care practice in Canada: a one-year, open-label, random-ized, comparative study of efficacy, safety, and cost-effectiveness. Clin Ther. 2001; 23:1492–507.
Article6. Gaston H, Absolon MJ, Thurtle OA, Sattar MA. Steroid re-sponsiveness in connective tissue diseases. Br J Ophthalmol. 1983; 67:487–90.
Article7. Munjal VP, Dhir SP, Jain IS. Steroid induced glaucoma. Indian J Ophthalmol. 1982; 30:379–82.8. Seiler T, Holschbach A, Derse M, et al. Complications of myopic photorefractive keratectomy with the excimer laser. Ophthalmology. 1994; 101:153–60.
Article9. Vetrugno M, Maino A, Quaranta G, Cardia L. A randomized, com-parative open-label study on the efficacy of latanoprost and timolol in steroid induced ocular hypertension after photorefractive keratectomy. Eur J Ophthalmol. 2000; 10:205–11.
Article10. Leibowitz HM, Ryan WJ Jr, Kupferman A. Comparative anti-in-flammatory efficacy of topical corticosteroids with low glauco-ma-inducing potential. Arch Ophthalmol. 1992; 110:118–20.
Article11. Sher NA, Chen V, Bowers RA, et al. The use of the 193-nm ex-cimer laser for myopic photorefractive keratectomy in sighted eyes: a multicenter study. Arch Ophthal. 1991; 109:1525–30.12. Johnson M, Kass MA, Moses RA, Grodzki WJ. Increased corneal thickness simulating elevated intraocular pressure. Arch Ophthalmol. 1978; 96:664–5.
Article13. Ehlers N, Bramsen T, Sperling S. Applanation tonometry and cen-tral corneal thickness. Acta Ophthalmol (Copenh). 1975; 53:34–43.
Article14. Shimizu K, Amano S, Tanaka S. Photorefractive keratectomy for myopia: one-year follow-up in 97 eyes. J Refract Corneal Surg. 1994; 10((2 Suppl)):S178–87.
Article15. Ishibashi T, Takagi Y, Mori K, et al. cDNA microarray analysis of gene expression changes induced by dexamethasone in cultured human trabecular meshwork cells. Invest Ophthalmol Vis Sci. 2002; 43:3691–7.16. Dickerson JE Jr, Steely HT Jr, English-Wright SL, Clark AF. The effect of dexamethasone on integrin and laminin expression in cul-tured human trabecular meshwork cells. Exp Eye Res. 1998; 66:731–8.17. Alward WL. The genetics of open-angle glaucoma: the story of GLC1A and myocilin. Eye (Lond). 2000; 14((Pt 3B)):429–36.
Article18. Alward WL, Fingert JH, Coote MA, et al. Clinical features asso-ciated with mutations in the chromosome 1 open-angle glaucoma gene (GLC1A). N Engl J Med. 1998; 338:1022–7.
Article19. Tang WC, Yip SP, Lo KK, et al. Linkage and association of my-ocilin (MYOC) polymorphisms with high myopia in a Chinese population. Mol Vis. 2007; 13:534–44.20. Zayats T, Yanovitch T, Creer RC, et al. Myocilin polymorphisms and high myopia in subjects of European origin. Mol Vis. 2009; 15:213–22.21. Machat JJ, Tayfour F. Photorefractive keratectomy for myopia: preliminary results in 147 eyes. Refract Corneal Surg. 1993; 9((2 Suppl)):S16–9.
Article22. Gartry DS, Kerr Muir MG, Marshall J. Excimer laser photo-refractive keratectomy. 18-month follow-up. Ophthalmology. 1992; 99:1209–19.23. Javadi MA, Mirbabaei-Ghafghazi F, Mirzade M, et al. Steroid in-duced ocular hypertension following myopic photorefractive keratectomy. J Ophthalmic Vis Res. 2008; 3:42–6.24. Fan DS, Yu CB, Chiu TY, et al. Ocular-hypertensive and anti-in-flammatory response to rimexolone therapy in children. Arch Ophthalmol. 2003; 121:1716–21.
Article25. Kohlhaas M, Boehm AG, Spoerl E, et al. Effect of central corneal thickness, corneal curvature, and axial length on applanation tonometry. Arch Ophthalmol. 2006; 124:471–6.
Article
