A Case of Traumatic Tricuspid Regurgitation Caused by Multiple Papillary Muscle Rupture
- Affiliations
-
- 1Department of Internal Medicine, Inje University College of Medicine, Pusan Paik Hospital, Busan, Korea. jsjang@medimail.co.kr
- 2Department of Internal Medicine, Inje University College of Medicine, Haeundae Paik Hospital, Busan, Korea.
- KMID: 2135433
- DOI: http://doi.org/10.4250/jcu.2011.19.1.41
Abstract
- Traumatic tricuspid regurgitation is a rare complication of blunt chest trauma. With the increase in the number of automobile accidents, traumatic tricuspid regurgitation has become an important problem after blunt chest trauma. It has been reported more frequently because of better diagnostic procedures and a better understanding of the pathology. The early diagnosis of traumatic tricuspid regurgitation is important because traumatic tricuspid injury could be effectively corrected with reparative techniques, early operation is considered to relieve symptoms and to prevent right ventricular dysfunction. Echocardiography can reveal the cause and severity of regurgitation. We experienced a case of tricuspid regurgitation after blunt chest trauma early diagnosis and valve repair were performed. This case reminds the physicians in the emergency department should be aware of this potential complication following non-penetrating chest trauma and echocardiography is useful and should play an early role.
MeSH Terms
Figure
-
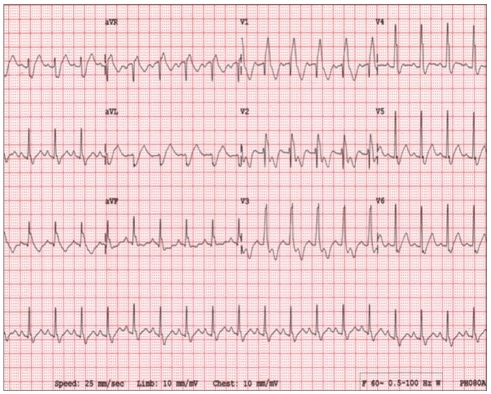
Fig. 1 The electrocardiogram showed complete right bundle branch block with posterior fascicular block.
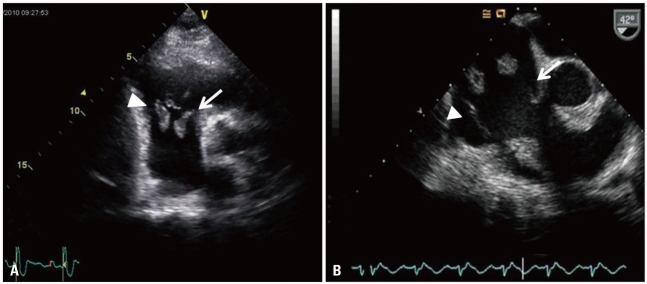
Fig. 2 The transthoracic echocardiography (A) and transesophageal echocardiography (B) showed prolapse of the septal (arrows) and anterior (arrow heads) tricuspid valve leaflet with large portions of the valve and the subvalvular appratus protruding into the right atrium indicating rupture of both anterior and posterior papillary muscle.
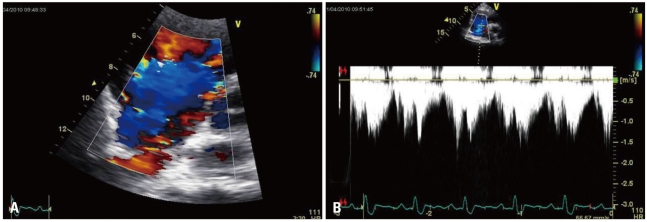
Fig. 3 The color-flow Doppler transthoracic echocardiography showed severe tricuspid regurgitation (A). Peak velocity of tricuspid valve was 1.62 m/sec and right ventricular systolic pressure was 20.5 mmHg (B).
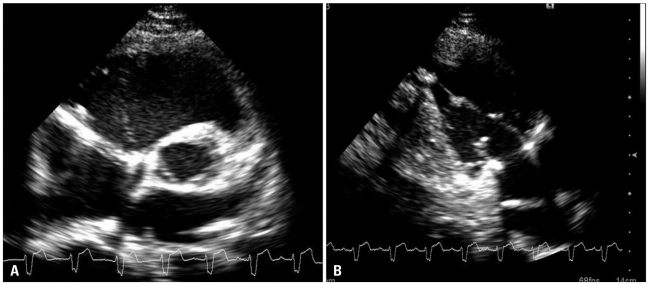
Fig. 4 The transthoracic echocardiography after tricuspid valve repair showed satisfactory leaflet coaptation (A) and repaired papillary muscle (B).
Reference
-
1. Schuster I, Graf S, Klaar U, Seitelberger R, Mundigler G, Binder T. Heterogeneity of traumatic injury of the tricuspid valve: A report of four cases. Wien Klin Wochenschr. 2008; 120:499–503. PMID: 18820855.2. Gayet C, Pierre B, Delahaye JP, Champsaur G, Andre-Fouet X, Rueff P. Traumatic tricuspid insufficiency. An underdiagnosed disease. Chest. 1987; 92:429–432. PMID: 3622022.3. Kim YJ, Moon KS, Kim JS, Hwang HK. Tricuspid insufficiency detected 8 years later following a blunt chest trauma. Korean Circ J. 1999; 29:1133–1137.4. Song HJ, Nam SH, Choi YJ, Park SH, Park SH, Han JJ. A case of native valve salvage for 8 years longstanding ruptured tricuspid valve after blunt chest trauma. Korean Circ J. 2004; 34:415–419.5. Lin SJ, Chen CW, Chou CJ, Liu KT, Su HM, Lin TH, Voon WC, Lai WT, Sheu SH. Traumatic tricuspid insufficiency with chordae tendinae rupture: a case report and literature review. Kaohsiung J Med Sci. 2006; 22:626–629. PMID: 17116624.6. Nelson M, Wells G. A case of traumatic tricuspid valve regurgitation caused by blunt chest trauma. J Am Soc Echocardiogr. 2007; 20:198.e4–198.e5. PMID: 17275711.7. Khurana S, Puri R, Wong D, Dundon BK, Brown MA, Worthley MI, Worthley SG. Latent tricuspid valve rupture after motor vehicle accident and routine echocardiography in all chest-wall traumas. Tex Heart Inst J. 2009; 36:615–617. PMID: 20069094.8. Bertrand S, Laquay N, El Rassi I, Vouhé P. Tricuspid insuffciency after blunt chest trauma in a nine-year-old child. Eur J Cardiothorac Surg. 1999; 16:587–589. PMID: 10609917.9. Richard P, Vayre F, Sabouret P, Gandjbakhch I, Ollivier JP. Outcome of traumatic tricuspid insufficiency, treated surgically. Apropos of 9 cases. Arch Mal Coeur Vaiss. 1997; 90:451–456. PMID: 9238461.10. Kulik A, Al-Saigh M, Yelle JD, Rubens FD. Subacute tricuspid valve rupture after traumatic cardiac and pulmonary contusions. Ann Thorac Surg. 2006; 81:1111–1112. PMID: 16488736.11. Maisano F, Lorusso R, Sandrelli L, Torracca L, Coletti G, La Canna G, Alfieri O. Valve repair for traumatic tricuspid regurgitation. Eur J Cardiothorac Surg. 1996; 10:867–873. PMID: 8911840.12. van Son JA, Danielson GK, Schaff HV, Miller FA Jr. Traumatic tricuspid valve insufficiency. Experience in thirteen patients. J Thorac Cardiovasc Surg. 1994; 108:893–898. PMID: 7967672.13. Bortolotti U, Scioti G, Milano A, Guglielmi C, Benedetti M, Tartarini G, Balbarini A. Post-traumatic tricuspid valve insufficiency. 2 cases of delayed clinical manifestation. Tex Heart Inst J. 1997; 24:223–225. PMID: 9339514.14. Yasuura K, Matsuura A, Maseki T, Miyahara K, Itoh T, Ichihara T, Sawazaki M. Successful repair of tricuspid regurgitation 46 years after causal blunt trauma. Scand J Thorac Cardiovasc Surg. 1996; 30:105–108. PMID: 8857685.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Post-traumatic tricuspid regurgitation with anterior papillary muscle rupture, corrected by papillary muscle reimplantation
- Traumatic Tricuspid Regurgitation Cause by Chordal Rupture: A Case Report
- Severe Tricuspid Regurgitation Following Blunt Chest Trauma - Successful Repair by PTFE Chordal Replacement and Ring Annuloplasty: A Case Report
- Successful Repair of Critical Tricuspid Regurgitation Secondary to a Ruptured Papillary Muscle in a Neonate
- Repair of Ruptured Papillary Muscle of the Tricuspid Valve as a Cause of Tricuspid Insufficiency Following Blunt Chest Trauma
