Anatomic Variants on Computed Tomography in Congenital Aural Atresia and Stenosis
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Dahua Hospital, Shanghai, China.
- 2Department of Otolaryngology-Head and Neck Surgery, Eye & ENT Hospital, Fudan University, Shanghai, China. ty.zhang2006@aliyun.com
- 3Research Center, Eye & ENT Hospital, Fudan University, Shanghai, China.
- KMID: 2128904
- DOI: http://doi.org/10.3342/ceo.2015.8.4.320
Abstract
OBJECTIVES
To quantitatively analyzing the anatomic variants on temporal computed tomography (CT) in congenital external auditory canal stenosis (EACS), congenital aural atresia (CAA), and normal ear structure.
METHODS
Through a retrospective study, we analyzed 142 temporal high-resolution CT studies performed in 71 microtia patients. The following 6 parameters were compared among the three groups: Marx classification, medial canal diameter, vertical facial nerve (VFN) anterior displacement, tegmen mastoideum position, tympanic cavity volume, and malleus-incus joint or malleus-incus complex (MIC) area.
RESULTS
The results showed that the microtia distributions in the Marx classification in these three groups were significantly different, as 86% (31 of 35) of ears with major microtia (third-degree dysplasia) had an atresia, and in 54.8% (23 of 42) of the minor microtic (first-degree or second-degree) ears, the bony or cartilaginous part of the external auditory canal was stenotic. Measurement data also showed that the potential medial canal diameter of the atresia group was obviously shorter than that of the stenosis group. The VFN anterior displacement and temporomandibular joint backward-shift together lead to medial canal diameters in ears with atresic canals that is smaller than those with stenotic canals. The tegmen mastoideum position was not significantly different between the three groups.
CONCLUSION
The mal-development of the external auditory canal is significantly associated with auricle and middle ear developmental anomalies. Compared with CAA ears, EACS have better development of the auricle, canal, tympanic cavity and MIC and relatively safer surgical operation except for the position of the tegmen mastoideum and the VFN.
MeSH Terms
Figure
-
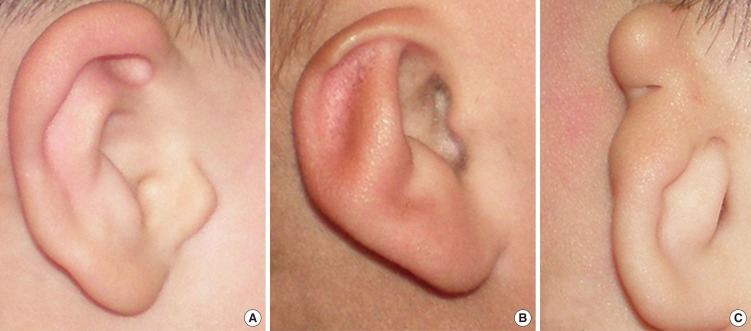
Fig. 1 Microtia. Grades I, II, and III in Marx classification are shown separately in panels (A), (B), and (C).

Fig. 2 Medial canal diameter. Right normal ear (A), right stenosis ear (B), and right atresia ear (C). The white line shows the tangent through the most salient point of the bone posterior wall of temporomandibular joint; the white arrow shows the vertical facial nerve.
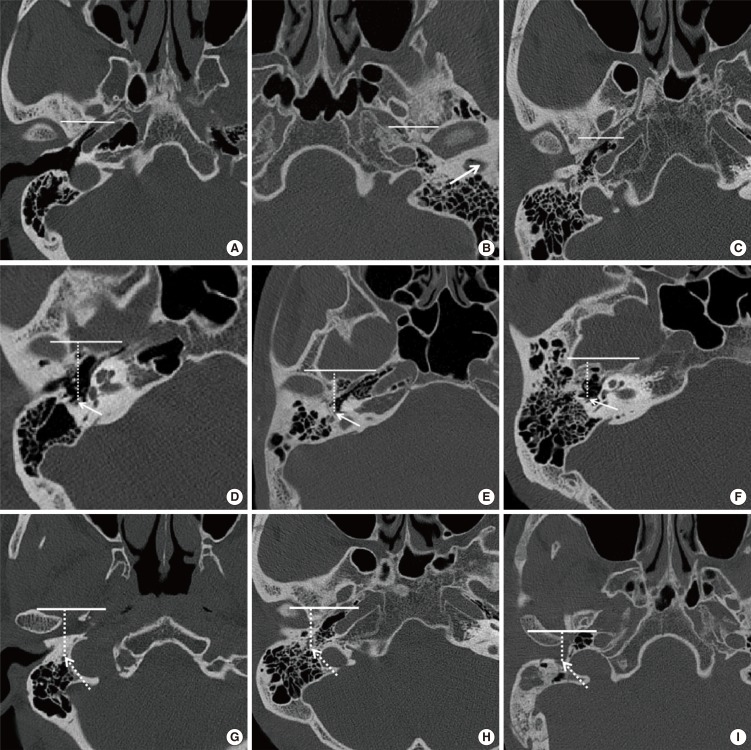
Fig. 3 Vertical facial nerve (VFN) position. The distance (dashed line) from the VFN to the coronal plane passing through the middle point of the foramen spinosum. Right normal ear (A, D, G), stenosis ear (B, E, H), right atresia ear (C, F, I). The line shows the horizontal line located in the coronal plane; the arrow shows stenosis of the canal in panel B and the starting point of the VFN in panels (D), (E), and (F); the dashed arrow shows the ending point of the VFN.

Fig. 4 Vertical facial nerve (VFN) antedisplacement. Computed tomography image at the level of the right round window niche (black arrow) shows an anteriorly displaced VFN (white arrow) which is normally positioned posterior to the round window niche (A, coronal plane; B, axial plane).

Fig. 5 The horizontal facial nerve (arrow) laterally displaces to the lateral wall of tympanic cavity in a left atretic ear. The ossicular is absent (A, axial plane; B, coronal plane).
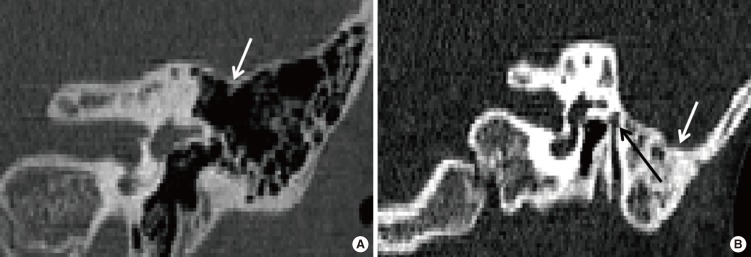
Fig. 6 Tegmen mastoideum position. (A) shows a normal tegmen mastoideum (white arrow) in left atretic ear; (B) shows an inferiorly displaced tegmen mastoideum (white arrow) and an anteriorly displaced facial nerve (black arrow) in the area of the oval window niche in a left atretic ear.
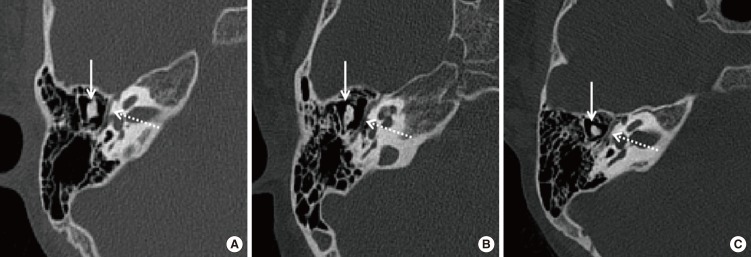
Fig. 7 Malleus-incus complex or malleus-incus joint in the axial plane in a normal canal (A), stenosis canal (B), and atresia canal (C). White dashed arrow shows the horizontal facial nerve and white solid arrow shows the malleus-incus complex or malleus-incus joint.
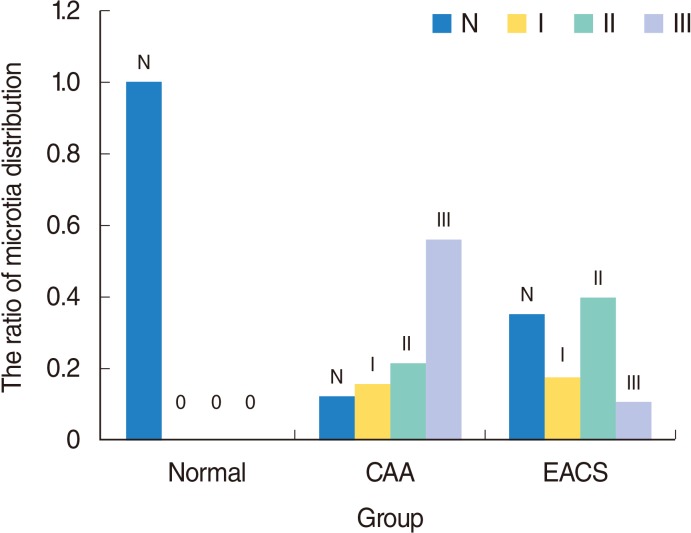
Fig. 8 The microtia distribution in Marx classification in the three groups. N represent normal auricle. Grades I, II, and III represent different deformity of auricle in Marx classification. CAA, congenital aural atresia; EACS, external auditory canal stenosis.
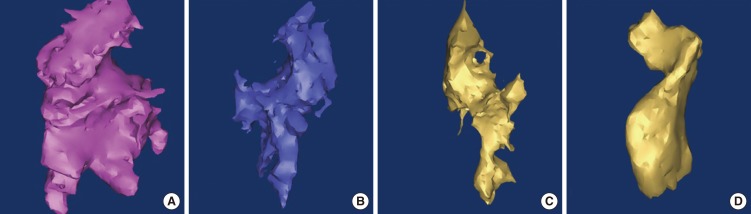
Fig. 9 Three-dimensional reconstruction tympanic cavity in left normal ear (A), in left stenosis ear (B), in left atresia ear (C, D).

Fig. 10 Comparison results of different parameters. Data are the mean±SD. MCD, medial canal diameter; VFN-FS, distance from vertical facial nerve (VFN) to the coronal plane through the middle point of foramen spinosum; LSCC-TM, distance from the middle point of lateral semicircular canal caliber to the tangent through the lowest point of tegmen mastoideum; TCV, tympanic cavity volume; MIC, malleus-incus complex; CAA, congenital aural atresia; EACS, external auditory canal stenosis. *P<0.05, statistical significance in pair-wise comparison. †The starting point of VFN. ‡The ending point of VFN.
Reference
-
1. Schuknecht HF. Congenital aural atresia. Laryngoscope. 1989; 9. 99(9):908–917. PMID: 2770382.
Article2. Jahrsdoerfer RA, Yeakley JW, Aguilar EA, Cole RR, Gray LC. Grading system for the selection of patients with congenital aural atresia. Am J Otol. 1992; 1. 13(1):6–12. PMID: 1598988.
Article3. Zhang TY, Li CL, Fu YY, Chi FL, Wang ZM. Management of congenital meatal stenosis and atresia: impact factors on long-term results and surgical strategy. Chin J Otol. 2012; 10(1):15–18.4. Klockars T, Rautio J. Embryology and epidemiology of microtia. Facial Plast Surg. 2009; 8. 25(3):145–148. PMID: 19809944.
Article5. Mukherji SK, Fatterpekar G, Castillo M, Stone JA, Chung CJ. Imaging of congenital anomalies of the branchial apparatus. Neuroimaging Clin N Am. 2000; 2. 10(1):75–93. PMID: 10658156.6. Kelley PE, Scholes MA. Microtia and congenital aural atresia. Otolaryngol Clin North Am. 2007; 2. 40(1):61–80. PMID: 17346561.
Article7. Benton C, Bellet PS. Imaging of congenital anomalies of the temporal bone. Neuroimaging Clin N Am. 2000; 2. 10(1):35–53. PMID: 10658154.8. Takegoshi H, Kaga K. Difference in facial canal anatomy in terms of severity of microtia and deformity of middle ear in patients with microtia. Laryngoscope. 2003; 4. 113(4):635–639. PMID: 12671419.
Article9. Lumbroso C, Sebag G, Argyropoulou M, Manach Y, Lallemand D. Preoperative X-ray computed tomographic evaluation of major aplasia of the ear in children. J Radiol. 1995; 4. 76(4):185–189. PMID: 7745552.10. Yuen HY, Ahuja AT, Wong KT, Yue V, van Hasselt AC. Computed tomography of common congenital lesions of the temporal bone. Clin Radiol. 2003; 9. 58(9):687–693. PMID: 12943639.
Article11. Yeakley JW, Jahrsdoerfer RA. CT evaluation of congenital aural atresia: what the radiologist and surgeon need to know. J Comput Assist Tomogr. 1996; Sep-Oct. 20(5):724–731. PMID: 8797901.
Article12. Fu Y, Zhang T. Facial nerve lying lateral to ossicles in one case of congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2011; 4. 75(4):597–599. PMID: 21281971.
Article13. Oliver ER, Lambert PR, Rumboldt Z, Lee FS, Agarwal A. Middle ear dimensions in congenital aural atresia and hearing outcomes after atresiaplasty. Otol Neurotol. 2010; 8. 31(6):946–953. PMID: 20684058.
Article14. Jahrsdoerfer RA, Garcia ET, Yeakley JW, Jacobson JT. Surface contour three-dimensional imaging in congenital aural atresia. Arch Otolaryngol Head Neck Surg. 1993; 1. 119(1):95–99. PMID: 8417750.
Article15. Swartz JD, Faerber EN. Congenital malformations of the external and middle ear: high-resolution CT findings of surgical import. AJR Am J Roentgenol. 1985; 3. 144(3):501–506. PMID: 3871559.
Article16. Yellon RF, Branstetter BF 4th. Prospective blinded study of computed tomography in congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2010; 11. 74(11):1286–1291. PMID: 20864187.
Article17. Dedhia K, Yellon RF, Branstetter BF, Egloff AM. Anatomic variants on computed tomography in congenital aural atresia. Otolaryngol Head Neck Surg. 2012; 8. 147(2):323–328. PMID: 22467282.
Article18. Shonka DC Jr, Livingston WJ 3rd, Kesser BW. The Jahrsdoerfer grading scale in surgery to repair congenital aural atresia. Arch Otolaryngol Head Neck Surg. 2008; 8. 134(8):873–877. PMID: 18711063.
Article19. Ikui A, Sando I, Haginomori S, Sudo M. Postnatal development of the tympanic cavity: a computer-aided reconstruction and measurement study. Acta Otolaryngol. 2000; 3. 120(3):375–379. PMID: 10894412.20. Hill CA, Richtsmeier JT. A quantitative method for the evaluation of three-dimensional structure of temporal bone pneumatization. J Hum Evol. 2008; 10. 55(4):682–690. PMID: 18715622.
Article21. Vrabec JT, Champion SW, Gomez JD, Johnson RF Jr, Chaljub G. 3D CT imaging method for measuring temporal bone aeration. Acta Otolaryngol. 2002; 12. 122(8):831–835. PMID: 12542201.
Article22. Osborn AJ, Oghalai JS, Vrabec JT. Middle ear volume as an adjunct measure in congenital aural atresia. Int J Pediatr Otorhinolaryngol. 2011; 7. 75(7):910–914. PMID: 21570132.
Article23. Leng TJ, Gong J, Lan BS. CT evaluation of malformed external and middle ear and its surgical correlation. Chin Med J (Engl). 1992; 6. 105(6):490–493. PMID: 1451550.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Functional and esthetic reconstruction of microtia and congenital aural atresia: a case report
- A Case of Image-Guided Surgery in Congenital Aural Atresia
- A case of congenital tricuspid stenosis
- Surgical Experiences of Congenital Aural Atresia Analysis of 53 Cases
- Congenital Aural Atresia Associated with Cholesteatoma
