Guide flange prosthesis for early management of reconstructed hemimandibulectomy: a case report
- Affiliations
-
- 1Department of Prosthodontics, Government Dental College and Hospital, Nagpur, Maharashtra, India. pravinandsmita@yahoo.co.in
- 2Department of Orthodontics and Dentofacial Orthopedics, SDKS Dental College and Hospital, Wanadongri, Nagpur, Maharashtra, India.
- KMID: 2118128
- DOI: http://doi.org/10.4047/jap.2011.3.3.172
Abstract
- Surgical resection of the mandible due to presence of benign or malignant tumor is the most common cause of the mandibular deviation. Depending upon the location and extent of the tumor in the mandible, various surgical treatment modalities like marginal, segmental, hemi, subtotal, or total mandibulectomy can be performed. The clinicians must wait for extensive period of time for completion of healing and acceptance of the osseous graft before considering the definitive prosthesis. During this initial healing period prosthodontic intervention is required for preventing the mandibular deviation. This case report describes early prosthodontic management of a patient who has undergone a reconstructed hemi-mandibulectomy with modified mandibular guide flange prosthesis. The prosthesis helps patient moving the mandible normally without deviation during functions like speech and mastication.
Keyword
MeSH Terms
Figure
-

Fig. 1 Pre-operative panoramic radiograph showing extensive radiolucent area in left mandible, B: Post-surgical panoramic radiograph showing reconstructed left mandible with osseous graft.

Fig. 2 Intraoral view showing loss of alveolar ridge on left side with vestibular obliteration. Note arrows indicating thick freely movable soft tissues. Note the deviation of the mandible on defect (left) side on opening.
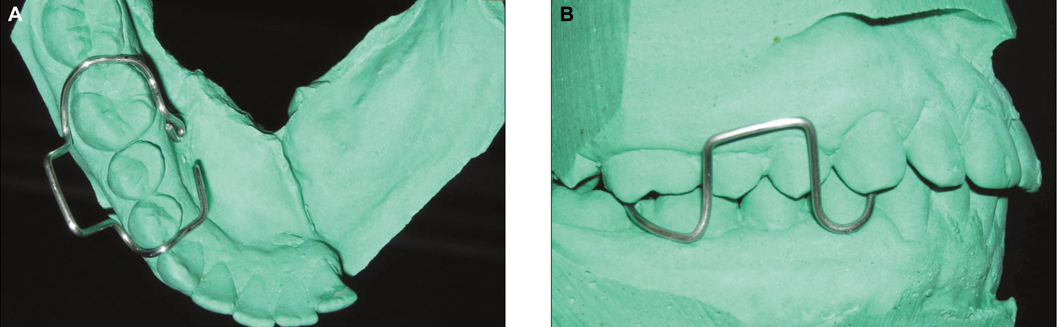
Fig. 3 A: Wire substructure: occlusal view, B: Wire substructure: buccal view.

Fig. 4 Completed modified guide flange prosthesis. Note arrows indicating the buccal indentations of opposing maxillary teeth in occlusion to guide the mandible in a definite closing point.

Fig. 5 Completed maxillary stabilization plate.

Fig. 6 A: Prosthesis in place during large mouth opening. Note occlusal extensions of the maxillary stabilization plate on right posteriors, B: Prosthesis during mandibular movements, C: Prosthesis guided the mandible in a definite closing point.
Reference
-
1. Shafer WG, Hine MK, Levy BM, Tomich CE. A textbook of oral pathology. 1993. 4th ed. Philadelphia: WB Saunders;86–229.2. Taylor TD. Taylor TD, editor. Diagnostic considerations for prosthodontic rehabilitation of the mandibulectomy patient. Clinical maxillofacial prosthetics. 2000. Chicago: Quintessence Publishing;155–170.3. Olson ML, Shedd DP. Disability and rehabilitation in head and neck cancer patients after treatment. Head Neck Surg. 1978. 1:52–58.4. Curtis DA, Plesh O, Miller AJ, Curtis TA, Sharma A, Schweitzer R, Hilsinger RL, Schour L, Singer M. A comparison of masticatory function in patients with or without reconstruction of the mandible. Head Neck. 1997. 19:287–296.5. Komisar A. The functional result of mandibular reconstruction. Laryngoscope. 1990. 100:364–374.6. Hidalgo DA. Fibula free flap: a new method of mandible reconstruction. Plast Reconstr Surg. 1989. 84:71–79.7. Hidalgo DA. Aesthetic improvements in free-flap mandible reconstruction. Plast Reconstr Surg. 1991. 88:574–585.8. Jewer DD, Boyd JB, Manktelow RT, Zuker RM, Rosen IB, Gullane PJ, Rotstein LE, Freeman JE. Orofacial and mandibular reconstruction with the iliac crest free flap: a review of 60 cases and a new method of classification. Plast Reconstr Surg. 1989. 84:391–403.9. Soutar DS, Widdowson WP. Immediate reconstruction of the mandible using a vascularized segment of radius. Head Neck Surg. 1986. 8:232–246.10. Matloub HS, Larson DL, Kuhn JC, Yousif NJ, Sanger JR. Lateral arm free flap in oral cavity reconstruction: a functional evaluation. Head Neck. 1989. 11:205–211.11. Marunick MT, Mathes BE, Klein BB. Masticatory function in hemimandibulectomy patients. J Oral Rehabil. 1992. 19:289–295.12. McConnel FM, Pauloski BR, Logemann JA, Rademaker AW, Colangelo L, Shedd D, Carroll W, Lewin J, Johnson J. Functional results of primary closure vs flaps in oropharyngeal reconstruction: a prospective study of speech and swallowing. Arch Otolaryngol Head Neck Surg. 1998. 124:625–630.13. Hsiao HT, Leu YS, Lin CC. Primary closure versus radial forearm flap reconstruction after hemiglossectomy: functional assessment of swallowing and speech. Ann Plast Surg. 2002. 49:612–616.14. McConnel FM, Teichgraeber JF, Adler RK. A comparison of three methods of oral reconstruction. Arch Otolaryngol Head Neck Surg. 1987. 113:496–500.15. Pauloski BR, Rademaker AW, Logemann JA, McConnel FM, Heiser MA, Cardinale S, Lazarus CL, Pelzer H, Stein D, Beery Q. Surgical variables affecting swallowing in patients treated for oral/oropharyngeal cancer. Head Neck. 2004. 26:625–636.16. Hsiao HT, Leu YS, Chang SH, Lee JT. Swallowing function in patients who underwent hemiglossectomy: comparison of primary closure and free radial forearm flap reconstruction with videofluoroscopy. Ann Plast Surg. 2003. 50:450–455.17. Wagner JD, Coleman JJ 3rd, Weisberger E, Righi PD, Radpour S, McGarvey S, Bayler A, Chen J, Crow H. Predictive factors for functional recovery after free tissue transfer oromandibular reconstruction. Am J Surg. 1998. 176:430–435.18. Garrett N, Roumanas ED, Blackwell KE, Freymiller E, Abemayor E, Wong WK, Gerratt B, Berke G, Beumer J 3rd, Kapur KK. Efficacy of conventional and implant-supported mandibular resection prostheses: study overview and treatment outcomes. J Prosthet Dent. 2006. 96:13–24.19. Desjardins RP. Laney WR, editor. Relating examination findings to treatment procedures. Maxillofacial prosthetics. 1979. Littleton: PSG Publishing;69–114.20. McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjian JH, Arbree NS. Classification system for partial edentulism. J Prosthodont. 2002. 11:181–193.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fabrication of functionally customized fixed prosthesis in a hemimandibulectomy patient with fibular graft using double scan technique: A case report
- Stent Flange-Induced Esophageal Stricture Treated with an Oral Steroid
- A Case of Management of an Inappropriate Penile Prosthesis
- Application of Goretex to Reconstruct Protrusion of the Prosthesis against Thin Tunicae Albuginea after Hydroflex Penile Prosthesis
- Anthropometric Study of Distal Femur & Compatibility of Gender Knee Prosthesis in Total Knee Replacement
