Subintimal Tracking and Re-entry (STAR) Technique with Contrast Guidance for Chronic Total Occlusion: Experience with 4 Cases
- Affiliations
-
- 1Department of Internal Medicine, Gwangju Veterans Hospital, Gwangju, Korea. gpkwy@naver.com
- 2Department of Internal Medicine, Yeosu Chonnam Hospital, Yeosu, Korea.
- KMID: 2116773
- DOI: http://doi.org/10.4068/cmj.2010.46.3.183
Abstract
- Percutaneous coronary intervention for chronic total occlusion of coronary arteries remains technically challenging. It shows lower procedural success rates compared with other lesion subsets. It is for this reason that interventional cardiologists have developed many techniques to recanalize chronically occluded arteries. Among them, we experienced some cases in which we used the subintimal tracking and re-entry (STAR) technique. Here we report our experience with a review of the literature.
MeSH Terms
Figure
-
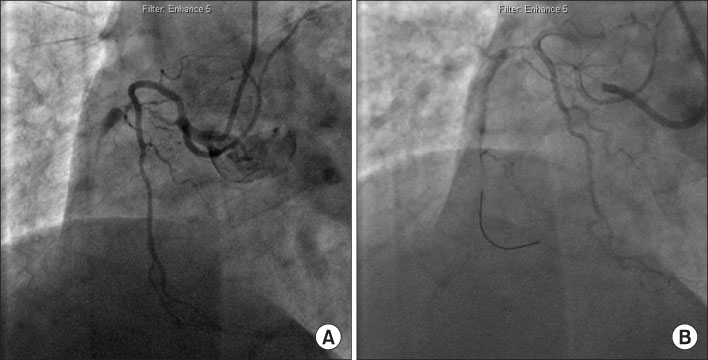
Fig. 1 First attempt at percutaneous coronary intervention for chronic total occlusion of the midportion of the right coronary artery in Case 1. (A) Right coronary angiogram showed significant stenosis of the proximal portion of the right coronary artery and chronic total occlusion of the midportion of the right coronary artery. (B) Attempt to cross the guidewire through the chronic total occlusion failed.

Fig. 2 Second attempt at percutaneous coronary intervention 6 months after the first attempt in Case 1. (A) Angiogram showed total occlusion of the midportion of the right coronary artery (star). (B) Retrograde intervention via the septal branch under contralateral contrast injection failed. (C) Guidewire passage via the antegrade approach failed. Note that the guidewire tip was outside the distal true lumen. (D) Subintimal tracking by contrast injection via microcatheter made the path to the distal true lumen (arrow). (E) Percutaneous transluminal coronary angioplasty was performed by using the anchor balloon technique after successful wiring into the distal true lumen. (F) Final angiogram after deployment of four sirolimus-eluting stents showed a good result without residual stenosis.
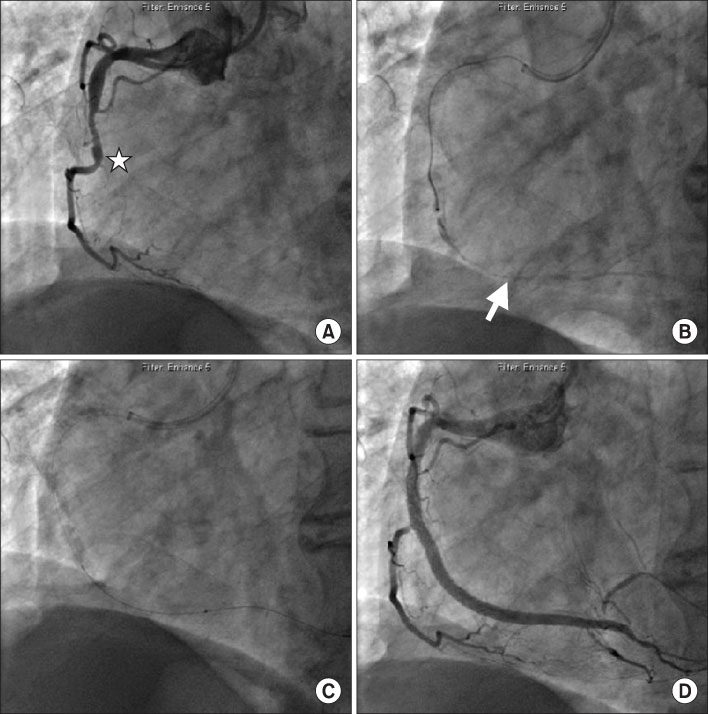
Fig. 3 Right coronary angiogram and percutaneous coronary intervention in Case 2. (A) Coronary angiogram showed total occlusion of the midportion of the right coronary artery at the takeoff of the side branch (star). (B) After subintimal tracking by contrast injection via microcatheter, the distal true lumen was visible (arrow). (C) Percutaneous transluminal balloon angioplasty was performed. (D) We obtained good results after deployment of three paclitaxel-eluting stents.
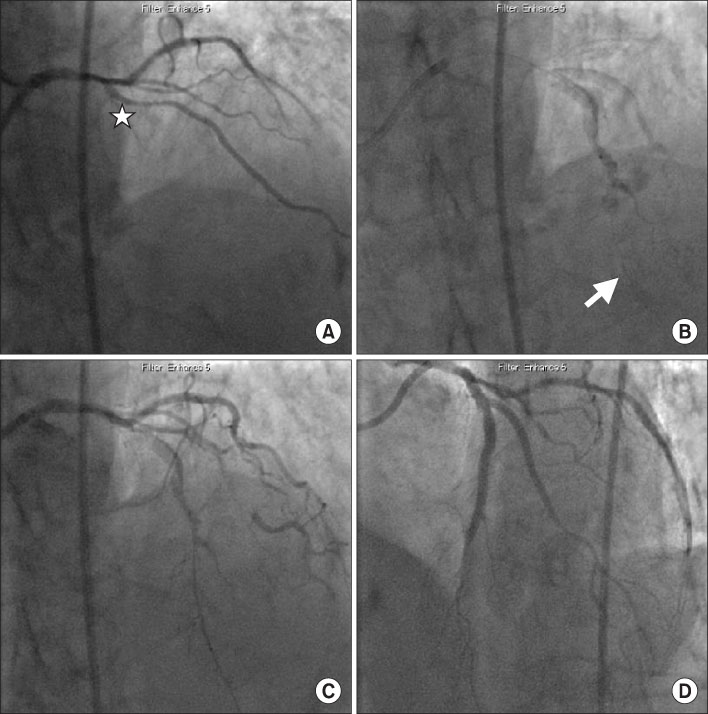
Fig. 4 Left coronary angiogram and percutaneous coronary intervention in Case 3. (A) Coronary angiogram showed total occlusion of the midportion of the left anterior descending coronary artery at the side branch (star). (B) After subintimal tracking by contrast injection via microcatheter, we could see the distal true lumen (arrow) with large dissection of the midportion of the left anterior descending coronary artery and diagonal branch. (C) The angiogram showed a good entrance of the guidewire into the distal true lumen. (D) Final angiogram revealed good distal flow without any complications after deployment of two paclitaxel-eluting stents for the left anterior descending coronary artery and one paclitaxel-eluting stent for the diagonal branch by kissing balloon angioplasty.

Fig. 5 Left coronary angiogram and percutaneous coronary intervention in Case 4. (A) Coronary angiogram revealed total occlusion of the distal portion of the left circumflex coronary artery at the side branch (star). (B) After contrast injection by use of a microcatheter, large dissection occurred. (C) Despite a visible distal true lumen (arrow), crossing the guidewire failed.
Reference
-
1. Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. 2005. 95:1088–1091.
Article2. Stone GW, Kandzari DE, Mehran R, Colombo A, Schwartz RS, Bailey S, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation. 2005. 112:2364–2372.
Article3. Stone GW, Reifart NJ, Moussa I, Hoye A, Cox DA, Colombo A, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part II. Circulation. 2005. 112:2530–2537.
Article4. Colombo A, Mikhail GW, Michev I, Iakovou I, Airoldi F, Chieffo A, et al. Treating chronic total occlusions using subintimal tracking and reentry: the STAR technique. Catheter Cardiovasc Interv. 2005. 64:407–411.
Article5. Carlino M, Godino C, Latib A, Moses JW, Colombo A. Subintimal tracking and re-entry technique with contrast guidance: a safer approach. Catheter Cardiovasc Interv. 2008. 72:790–796.
Article6. Erlich I, Strauss BH, Butany J. Stent thrombosis following the STAR technique in a complex RCA chronic total occlusion. Catheter Cardiovasc Interv. 2006. 68:708–712.
Article7. Schwartz RS, Chronos NA, Virmani R. Preclinical restenosis models and drug-eluting stents: still important, still much to learn. J Am Coll Cardiol. 2004. 44:1373–1385.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reverse Controlled Antegrade and Retrograde Subintimal Tracking in Chronic Total Occlusion of Right Coronary Artery
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- The Outback(R) LTDtrade mark Catheter: The Novel Re-Entry Technique in Recanalization of Chronic Inflow Occlusion of the Superficial Femoral Arteries in 3 Cases
- Successful Recanalization of a Long Superficial Femoral Artery Occlusion by Retrograde Subintimal Angioplasty After a Failed Antegrade Subintimal Approach
- Procedural and Early Outcomes of Two Re-entry Devices for Subintimal Recanalization of Aortoiliac and Femoropopliteal Chronic Total Occlusions
