A Case of Lipoid Pneumonia Associated with Silicon Oil Injection into Breast
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University School of Medicine, Cheongju, Korea. drahnjy@chungbuk.ac.kr
- 2Department of Internal Medicine, The Cheongju St. Mary's Hospital, Cheongju, Korea.
- 3Chungcheong Respiratory Institute, Cheongju, Korea.
- KMID: 2114624
- DOI: http://doi.org/10.4046/trd.2010.69.4.288
Abstract
- Exogenous lipoid pneumonia occurs rarely in healthy people. In most cases, exogenous lipoid pneumonia is usually caused by aspiration of mineral, vegetable, or animal oil. We report the case of 42-year-old woman, who have experienced lipoid pneumonia after silicon injection into her breast for cosmetic purposes. The patient experienced fever, dyspnea, sputum, and hemoptysis after silicon injection into her breast. Chest computed tomography demonstrated non-segmental distribution of bilateral consolidation in both lung fields. A transbronchial lung biopsy specimen shows foamy microphages in alveolar spaces. Papanicolaous staining of bronchoalveolar lavage fluid showed abundant foamy marcrophages and many neutrophils. With these results, we confirmed lipoid pneumonia was associated with silicon oil injection into breast.
Keyword
MeSH Terms
Figure
-

Figure 1 Chest radiography in a 42-year-old woman with hemoptysis and dyspnea. (A) The initial chest PA shows ill defined consolidation in both middle and lower lung field. (B) Chest lateral radiography shows main haziness in anterior portion of lung. (C) In admission 8 days later, chest PA shows improving of consolidation in both middle and lower luing field.
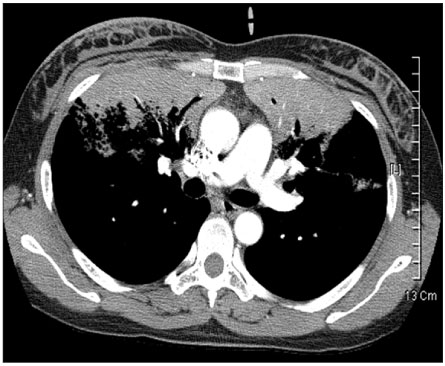
Figure 2 Chest CT shows non-segmental distribution of bilateral consolidation in both lung field.
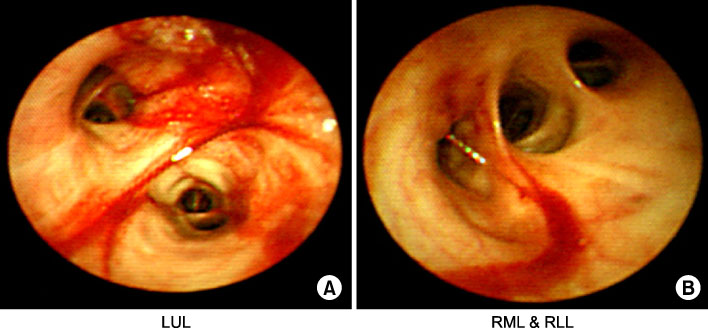
Figure 3 Bronchoscopic findings. Bronchoscope shows mucosal edema, flush, bleeding in left upper lobe (LUL) bronchus (A) and right middle lobe (RML) and right lower lobe (RLL) bronchus (B).
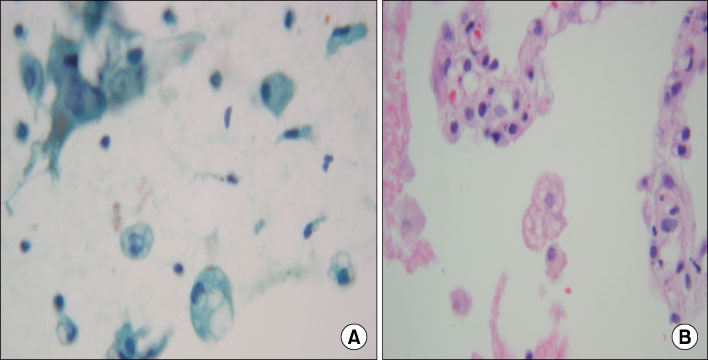
Figure 4 TBLB and BAL fluid slide. (A) TBLB shows foamy macrophage in alveolar spaces (H&E stain, ×40). (B) Papanicolaous staining of bronchoalveolar lavage fluid shows abundant foamy marcrophage and mixed with many neutrophils (cytospin preparation; ×40).
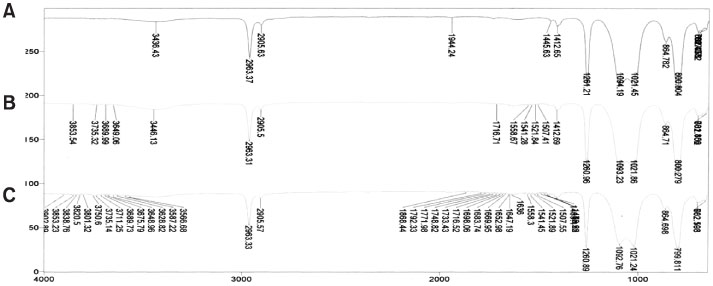
Figure 5 Chemical analysis by FTIR and Pyrolyzer-Gas chromatography. It means almost same material among three specimen. (A) General sylicon oil. (B) Injection oil to patient. (C) Tissue extract from patient.
Reference
-
1. Gondouin A, Manzoni P, Ranfaing E, Brun J, Cadranel J, Sadoun D, et al. Exogenous lipid pneumonia: a retrospective multicentre study of 44 cases in France. Eur Respir J. 1996. 9:1463–1469.2. Spickard A 3rd, Hirschmann JV. Exogenous lipoid pneumonia. Arch Intern Med. 1994. 154:686–692.3. Shin DJ, Park BS, Yang MS, Han HS, Koh YY, Moon HR, et al. Clinical study on lipoid pneumonia caused by aspiration of squalene. J Korean Pediatr Soc. 1991. 34:654–661.4. Edgerton MT, Wells JH. Indications for and pitfalls of soft tissue augmentation with liquid silicone. Plast Reconstr Surg. 1976. 58:157–165.5. Coulaud JM, Labrousse J, Carli P, Galliot M, Vilde F, Lissac J. Adult respiratory distress syndrome and silicone injection. Toxicol Eur Res. 1983. 5:171–174.6. Ellenbogen R, Rubin L. Injectable fluid silicone therapy. Human morbidity and mortality. JAMA. 1975. 234:308–309.7. Rodríguez MA, Martínez MC, Lopez-Artíguez M, Soria ML, Bernier F, Repetto M. Lung embolism with liquid silicone. J Forensic Sci. 1989. 34:504–510.8. Chastre J, Basset F, Viau F, Dournovo P, Bouchama A, Akesbi A, et al. Acute pneumonitis after subcutaneous injections of silicone in transsexual men. N Engl J Med. 1983. 308:764–767.9. Barie PS, Malik AB. Role of intravascular coagulation and granulocytes in lung vascular injury after bone marrow embolism. Circ Res. 1982. 50:830–838.10. Idell S, James KK, Gillies C, Fair DS, Thrall RS. Abnormalities of pathways of fibrin turnover in lung lavage of rats with oleic acid and bleomycin-induced lung injury support alveolar fibrin deposition. Am J Pathol. 1989. 135:387–399.11. Abraham E. Coagulation abnormalities in acute lung injury and sepsis. Am J Respir Cell Mol Biol. 2000. 22:401–404.12. Lee KS, Müller NL, Hale V, Newell JD Jr, Lynch DA, Im JG. Lipoid pneumonia: CT findings. J Comput Assist Tomogr. 1995. 19:48–51.13. Laurent F, Philippe JC, Vergier B, Granger-Veron B, Darpeix B, Vergeret J, et al. Exogenous lipoid pneumonia: HRCT, MR, and pathologic findings. Eur Radiol. 1999. 9:1190–1196.14. Silverman JF, Turner RC, West RL, Dillard TA. Bronchoalveolar lavage in the diagnosis of lipoid pneumonia. Diagn Cytopathol. 1989. 5:3–8.15. Hyun JG, Rhee CH. Clinical investigation of lipoid pneumonia in adults. Tuberc Respir Dis. 1996. 43:965–975.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Lipoid Pneumonia Induced by Aspiration of Shark Liver Oil
- A Case of Lipoid Pneumonia Caused by Aspiration of Laxatives
- A Case of Lipoid Pneumonia after Ingestion of Green Perilla Oil
- A Case of Lipoid Pneumonia Induced by Aspiration of Shark Liver Oil
- Experimental Study on Shark Liver Oil-Induced Lipoid Pneumonia in Rats
