J Korean Ophthalmol Soc.
2009 Mar;50(3):347-352. 10.3341/jkos.2009.50.3.347.
Comparison of Clinical Results Between OZil(R) Mode and Hyperpulse Mode in Phacoemulsification
- Affiliations
-
- 1Department of Ophthalmology, College of Medicine, The Catholic University of Korea, Seoul, Korea. sara514@catholic.ac.kr
- KMID: 2111243
- DOI: http://doi.org/10.3341/jkos.2009.50.3.347
Abstract
-
PURPOSE: To compare the intraoperative and short term postoperative outcomes of cataract surgery performed with custom pulse mode of OZil(R) and hyperpulse mode of conventional phacoemulsification
METHODS
The patients underwent cataract surgery using the OZil(R) custom pulse mode phacoemulsification (Group 1, n=30) or the conventional phaco Hyperpulse mode one (Group 2, n=36) of Infiniti Vision System. Mean ultrasound time, CDE (Cumulated dissipated energy) and total BSS volume were measured during operation. Best corrected visual acuity, central corneal thickness and endothelial cell counts were checked on 1 day, 1 momth, 2 months after surgery.
RESULTS
CDE was decreased significantly in group 1 (p<0.05). But, there were no significant differences in two groups of the mean ultrasound time and the BSS volume (p>0.05). At 2 months, the endothelial thickness was 552.94+/-27.95 micrometer in group 1, and 568.00+/-31.22 micrometer in group 2 and the endothelial cell counts was 2683.0+/-235.6 cell/mm2 and 2694.2+/-407.9 cell/mm2, respectatively. There were no significant differences in two groups.
CONCLUSIONS
The OZil(R) custom pulse mode phacoemulsification is an effective procedure in cataract surgery as much as the conventional hyperpulse mode phacoemulsification.
Figure
-
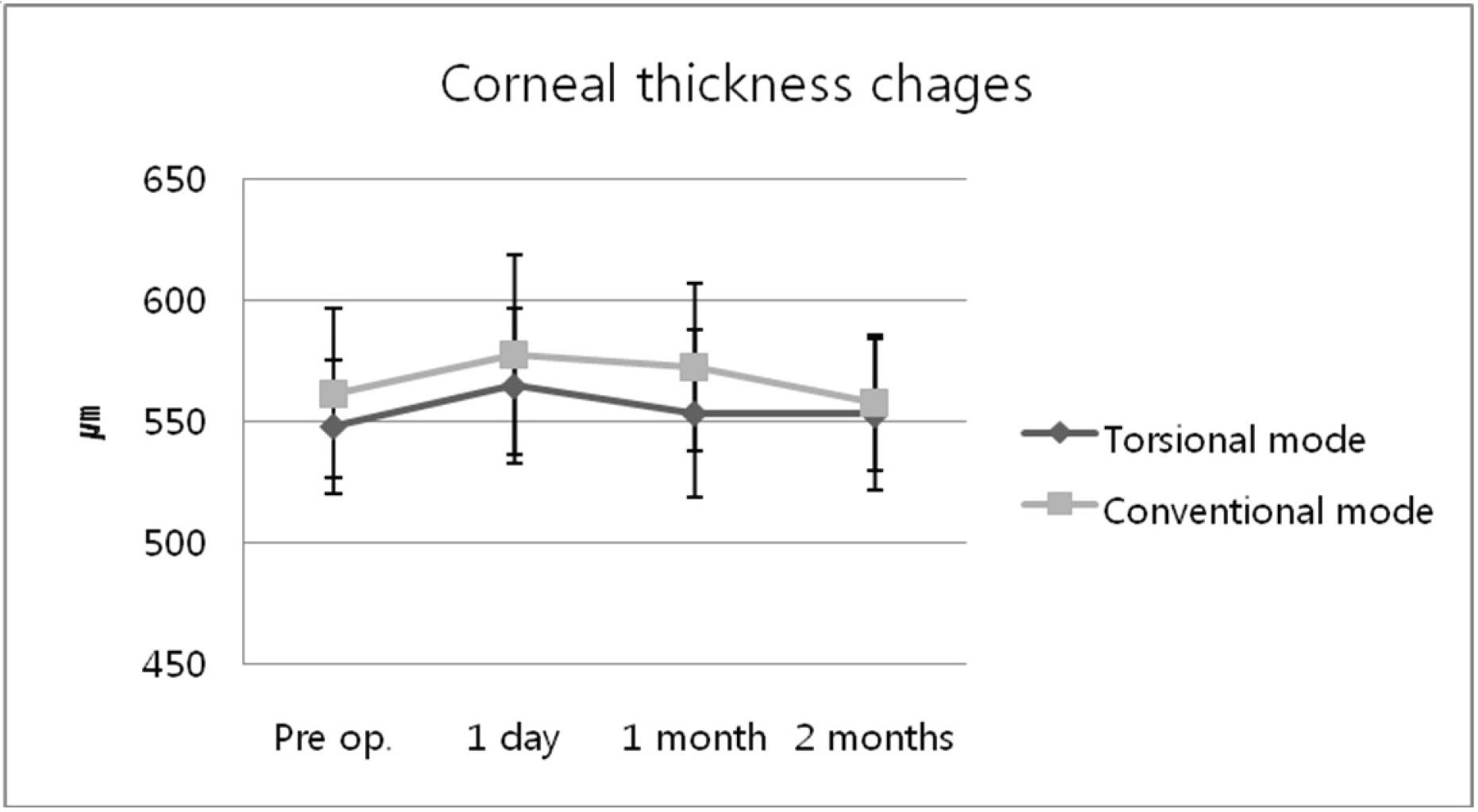
Figure 1. Corneal thickness in 2 groups. there is no statistically significant difference between the two groups (p>0.05). Group 1=OZil® custom pulse mode phacoemulsification; Group 2=Hyperpulse mode phaco-emulsification.

Figure 2. Postoperative Changes in endothelial cell count (cell/mm2). Group 1=OZil® custom pulse mode phacoemulsification; Group 2=Hyperpulse mode phaco-emulsification.

Figure 3. Endothelial cell count change in two groups. The mean endothelial cell counts decreased 5.14% in torsional phacoemulsification and 7.07% in conventional phacoemulsification at 60 days, respectively. Group 1=OZil® custom pulse mode phacoemulsification; Group 2=Hyperpulse mode phacoemulsification.
Reference
-
References
1. Vargas LG, Holzer MP, Solomon KD, et al. Endothelial cell integrity after phacoemulsification with 2 different handpieces. J Cataract Refract Surg. 2004; 30:478–82.
Article2. O'Brien PD, Fitzpatrick P, Kilmartin DJ, Beatty S. Risk factors for endothelial cell loss after phacoemulsification surgery by a junior resident. J Cataract Refract Surg. 2004; 30:839–43.3. Rho CR, Kim SY, Joo CK. Clinical Result of Cataract Operation using Custom Control Software. J Korean Ophthalmol Soc. 2006; 47:735–39.4. Liu Y, Zeng M, Liu X, et al. Torsional mode versus conventional ultrasound mode phacoemulsification: randomized comparative clinical study. J Cataract Refract Surg. 2007; 33:287–92.5. Chylack LT Jr, Leske MC, McCarthy D. Lens Opacities Classification System II (LOCS II). Arch Ophthalmol. 1989; 107:991–7.
Article6. Vasavada V, Vasavada V, Raj SM, Vasavada AR. Intraoperative performance and postoperative outcomes of microcoaxial phacoemulsification: Observational study. J Cataract Refract Surg. 2007; 33:1019–24.7. Kelman CD. Phaco-emulsification and aspiration. A new technique of cataract removal. A preliminary report. Am J Ophthalmol. 1967; 64:23–35.8. Polack FM, Sugar A. The phacoemulsification procedure Ⅲ corneal complications. Invest Ophthalmol Vis Sci. 1977; 16:39–46.9. Gwin RM, Warren JK, Samuelson DA, Gum GG. Effects of phacoemulsification and extracapsular lens removal on corneal thickness and endothelialcell density in the dog. Invest Ophthalmol Vis Sci. 1983; 24:227–36.10. Strobel J, Jacobi KW. Phacoemulsification and planed ECCE: Intraoperative differences in intraocular heating. Eur J Implant Refract Surg. 1991; 3:135–8.11. Gil SY, Kang SB, Lee SH, Chung SK. The Effect of Phaco-emulsification with Oscillation Device on the Cornea and Lens Opcatiy. J Korean Ophthalmol Soc. 2007; 47:1948–53.12. Kim HJ, Kim JH, Lee DH. Coaxial phacoemulsification, Corneal endothelial cell damage, Microincision cataract surgery. J Korean Ophthalmol Soc. 2007; 48:19–26.13. Hoffman RS, Fine IH, Packer M, Brown LK. Comparison of sonic and ultrasonic phacoemulsification using the Staar Sonic Wave system. J Cataract Refract Surg. 2002; 28:1581–4.
Article14. Mackool RJ, Brint SF. AquaLase: a new technology for cataract extraction. Curr Opin Ophthalmol. 2004; 15:40–3.
Article15. Vasavada AR, Raj SM, Lee YC. NeoSoniX ultrasound versus ultrasound alone for phacoemulsification; randomized clinical trial. J Cataract Refract Surg. 2004; 30:2332–5.16. Seibel RS. Phacodynamics: Mastering the tools and techniques of phacoemulsification sergery. 4th ed.Los Angeles: SLACK;2005. p. 122–3.17. Braga-Mele R. Thermal effect of microburst and hyperpulse settings during sleeveless bimanual phacoemulsification with advanced power modulations. J Cataract Refract Surg. 2006; 32:639–42.
Article18. Alio J, Rodriguez-Prats JL, Galal A, Ramzy M. Outcomes of microincision cataract versus coaxial phacoemulsification. Ophthalmology. 2005; 112:1997–2003.19. Cameron MD, Poyer JF, Aust SD. Identification of free radicals produced during phacoemulsification. J Cataract Refract Surg. 2001; 27:463–70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influences on Astigmatism and Corneal Endothelium Using Two Different Incision Sizes and Mode of Phacoemulsification
- Clinical Result of Cataract Operation using Custom Control Software
- Comparison of Surgical Results between WhiteStar Mode and Continuous Mode in the Phacoemulsification Unit
- Comparison of Influences on the Cornea between the WhiteStar Mode and Continuous Mode
- Comparison of Clinical Results between Ellips and Ozil Modes in Phacoemulsification
