J Korean Orthop Assoc.
2013 Feb;48(1):9-15. 10.4055/jkoa.2013.48.1.9.
Intercalary Allograft Reconstruction after Malignant Tumor Resection around the Knee
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. hankim@snu.ac.kr
- 2Orthopaedic Oncology Clinic, National Cancer Center, Goyang, Korea.
- KMID: 2106657
- DOI: http://doi.org/10.4055/jkoa.2013.48.1.9
Abstract
- PURPOSE
We aimed to assess the treatment outcomes and factors affecting bone union of intercalary allograft reconstruction after primary malignant bone tumor resection around the knee.
MATERIALS AND METHODS
Twenty-one patients who underwent intercalary allograft reconstruction after resection of a malignant tumor of femur or tibia were retrospectively reviewed. The average follow-up period was 46.4 months. Location of the tumor was as follows: femur in 12 cases and tibia in 9. Osteosarcoma was the most common tumor (12 cases). Intercalary allograft was internally fixed with an intramedullary (IM) nail in 3 cases, with a plate in 12 cases and with an IM nail combined with a plate in 6 cases. The survival of the grafts and functional outcomes were evaluated. Factors affecting bone union and complications were assessed.
RESULTS
All allografts survived without removal. The average Musculoskeletal Tumor Society functional score was 27. The mean length of the allograft was 16.7 cm and bony union took 10.9 months, in average. Nonunion occurred in 6 cases: at the diaphyseal side in 3, and the remaining 3 at the metaphyseal side. The graft length was shorter than average in all the diaphyseal side nonunion cases and longer than average in all the metaphyseal side nonunion cases. All cases of nonunion obtained bone union after additional operations (autologous bone graft alone: 1, bone graft with hardware change: 5).
CONCLUSION
Survival and functional outcomes of intercalary allograft were satisfactory. Long allograft showed a tendency of fracture or nonunion at the metaphyseal side. Nonunion could be managed with additional operation without allograft removal.
MeSH Terms
Figure
-
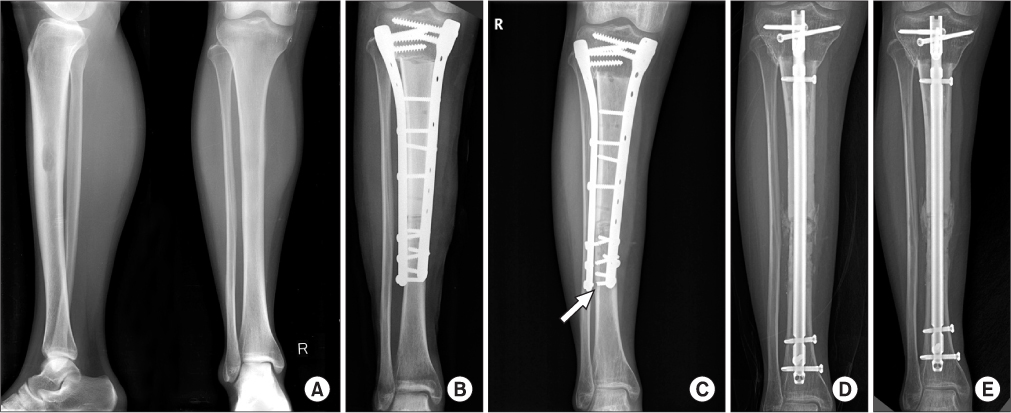
Figure 1 (A, B) This patient underwent wide excision and intercalary reconstruction with allograft due to ewing's sarcoma. (C) Nonunion of diaphyseal junction and screw breakage (arrow) were noted at 9 months postoperatively. (D) Removal of plates, autogenous bone graft and intramedullary nailing were performed. (E) Bony union was identified after 12 months.
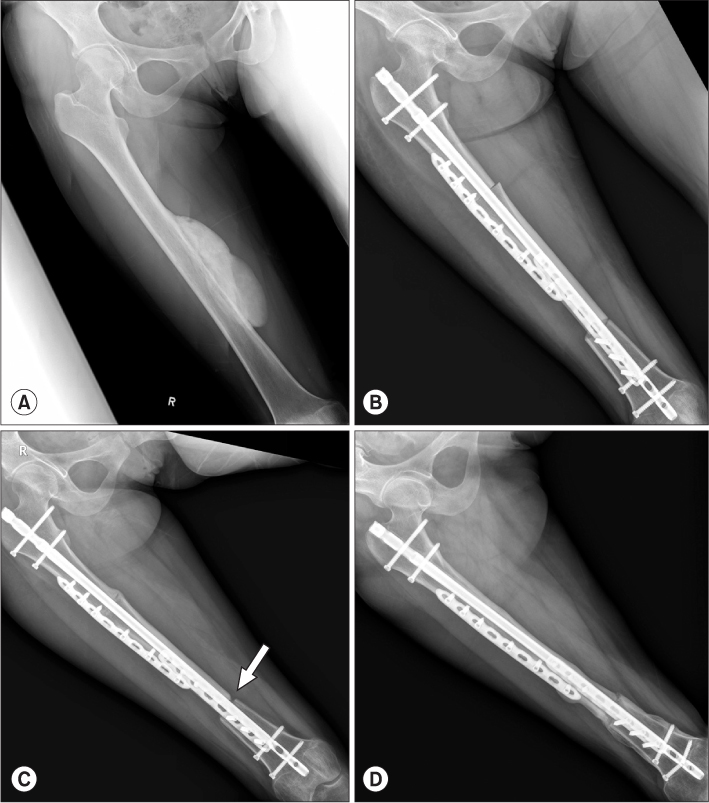
Figure 2 (A, B) This patient underwent intercalary resection and reconstruction with allograft and intramedullary nail due to parosteal osteosarcoma. (C) Nounion (arrow) was noted at 10 months postoperatively. (D) Bony union was achieved by autologous bone graft at 12 months.
Reference
-
1. Weber KL. What's new in musculoskeletal oncology. J Bone Joint Surg Am. 2005. 87:1400–1410.
Article2. Muscolo DL, Ayerza MA, Aponte-Tinao L, Ranalletta M, Abalo E. Intercalary femur and tibia segmental allografts provide an acceptable alternative in reconstructing tumor resections. Clin Orthop Relat Res. 2004. 426:97–102.
Article3. Frisoni T, Cevolani L, Giorgini A, Dozza B, Donati DM. Factors affecting outcome of massive intercalary bone allografts in the treatment of tumours of the femur. J Bone Joint Surg Br. 2012. 94:836–841.
Article4. Fuchs B, Ossendorf C, Leerapun T, Sim FH. Intercalary segmental reconstruction after bone tumor resection. Eur J Surg Oncol. 2008. 34:1271–1276.
Article5. Rose PS, Shin AY, Bishop AT, Moran SL, Sim FH. Vascularized free fibula transfer for oncologic reconstruction of the humerus. Clin Orthop Relat Res. 2005. 438:80–84.
Article6. Mankin HJ, Springfield DS, Gebhardt MC, Tomford WW. Current status of allografting for bone tumors. Orthopedics. 1992. 15:1147–1154.
Article7. Mankin HJ, Gebhardt MC, Jennings LC, Springfield DS, Tomford WW. Long-term results of allograft replacement in the management of bone tumors. Clin Orthop Relat Res. 1996. 324:86–97.
Article8. Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993. 286:241–246.
Article9. Ahlmann ER, Menendez LR. Intercalary endoprosthetic reconstruction for diaphyseal bone tumours. J Bone Joint Surg Br. 2006. 88:1487–1491.
Article10. Chen TH, Chen WM, Huang CK. Reconstruction after intercalary resection of malignant bone tumours: comparison between segmental allograft and extracorporeally-irradiated autograft. J Bone Joint Surg Br. 2005. 87:704–709.11. Thompson RC Jr, Pickvance EA, Garry D. Fractures in large-segment allografts. J Bone Joint Surg Am. 1993. 75:1663–1673.
Article12. Aponte-Tinao L, Farfalli GL, Ritacco LE, Ayerza MA, Muscolo DL. Intercalary femur allografts are an acceptable alternative after tumor resection. Clin Orthop Relat Res. 2012. 470:728–734.
Article13. Vander Griend RA. The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am. 1994. 76:657–663.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bone Reconstruction: Structural Allograft and Autograft
- Limb Salvage Surgery Using Whole Knee Joint Allograft Reconstruction in Osteosarcoma
- Low-heat Treated Intercalary Autograft Reconstruction in Limb Salvage of Primary Malignant Bone Tumor
- Resection, Reconstruction and Functional Result for Malignant Neoplasm of Humerus
- Allograft Reconstruction Following the Segmental Resection of Malignant Bone Tumors in the Long Bones
