Upper Airway Obstruction Caused by Intratracheal Ectopic Thyroid Tissue during Pregnancy
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Sungkyunkwan University School of Medicine, Korea.
- 2Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- KMID: 2100475
- DOI: http://doi.org/10.3803/jkes.2005.20.4.413
Abstract
- Herein is report an extremely rare case of an intratracheal ectopic thyroid gland related with pregnancy. A 34-year-old woman, in gestational week 11, presented with stridor, progressive dyspnea and a choking sensation during her second pregnancy. Computed tomography of the neck and chest revealed a round intratracheal mass obstructing the airway. A bronchoscopic biopsy with LASER cauterization was performed, and the histological finding revealed normal thyroid tissue. The external thyroid of the patient was evaluated, but only found benign nodules in the thyroid gland. She underwent a segmental resection of the trachea, including the mass and the 1st tracheal cartilage. The histological findings revealed the intratracheal mass to be composed of benign thyroid tissue with nodular hyperplasia. After surgery, no pulmonary symptoms were evident. This case suggested the effect of pregnancy on thyroid tissue stimulatied due to a combination of an increasing human chorionic gonadotropin(hCG) level and relative iodine deficiency during pregnancy. This is the first report on the detection of intratracheal ectopic thyroid tissue during pregnancy in Korea.
MeSH Terms
Figure
-

Fig. 1 Lateral view of the neck shows a discrete, sharply defined, rounded lesion that narrows airway.
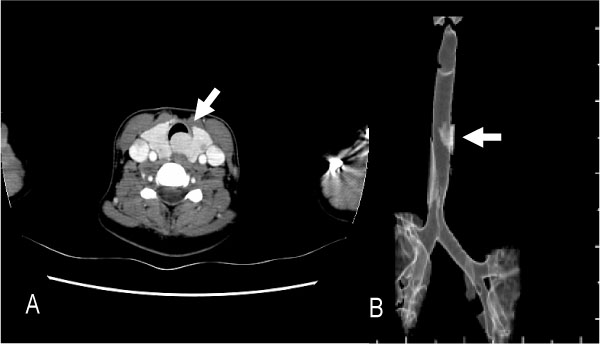
Fig. 2 A. Neck CT scan shows a 2.1 cm-sized round lesion arising from the postero-lateral wall of the subglottic trachea and the airway at the level of the lesion is near totally occluded. B. Sagittal view of the airway shows small extraluminal component that is connected with intraluminal lesion.

Fig. 3 Thyroid sonography shows a 0.6 cm-sized low echoic nodule with internal calcification, and 0.7 cm-sized nonspecific low echoic nodule and 0.4 cm-sized cyst are also detected.
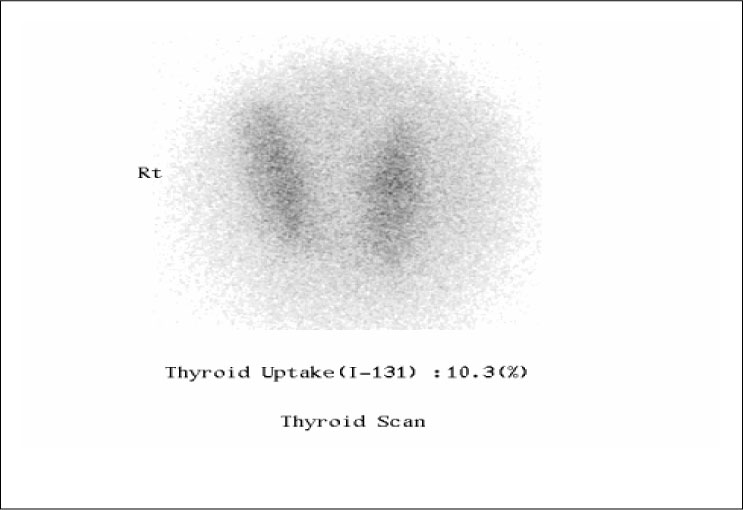
Fig. 4 I131 thyroid scan shows mildly enlarged thyroid gland with heterogeneous radioiodine uptake (10.3%). The scan do not show any lesion of abnormal radioiodine uptake.
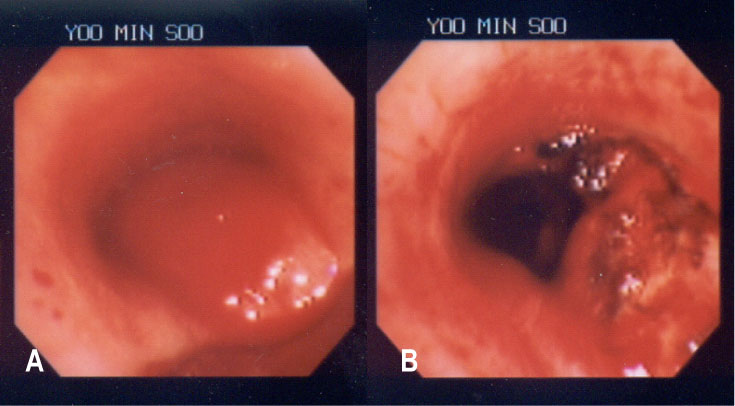
Fig. 5 A. Upper trachea is almost completely obstructed by round mass with smooth surface covered by intact mucosa. This mass is located 2 cm distal to vocal cord on the left posterolateral wall of trachea. B. Dilated tracheal lumen is seen after mass resection using LASER cauterization.
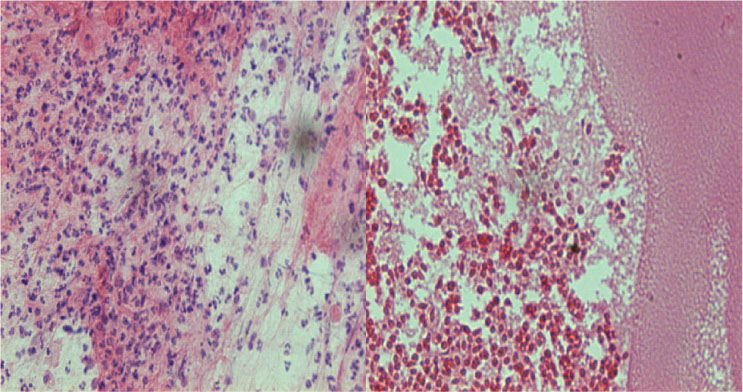
Fig. 6 Fine needle aspiration biopsy of thyroid nodule shows several small follicles and colloid material, favoring nodular hyperplasia.

Fig. 7 A. Gross finding of segmental resection of trachea shows homogenous yellow and whitish intraluminal polypoid mass, growing from external area of trachea to lumen. B. The microscopic finding shows that the mass shows thyroid follicles with nodular hyperplasia. Note the thyroid cartilage adjacent to the thyroid follicles. (H&E, ×100)
Reference
-
2. Dowling EA, Johson IM, Collier FCD, Dillard RA. Intratracheal goiter: a clinico-pathologic review. Ann Surg. 1962. 156:258–267.3. Byrd MC, Thompson LD, Wieneke JA. Intratracheal thyroid tissue: a case report and literature review. Ear Nose Throat. 2003. 82:514–518.4. Randolph J, Grunt JA, Vawter GF. The medical and surgical Aspects of intratracheal goiter. N Engl J Med. 1963. 268:457–461.5. Myers EN, Pantangco IP. Intratracheal thyroid. Laryngoscope. 1975. 85:1833–1840.6. Konstantinos NK, charanjeit SU, john PD. Benign intratracheal thyroid tissue: a rare cause of upper airway obstruction. Interactive Cardiovascular and Thoracic Surgery. 2003. 2:644–646.7. Dossing H, Jorgensen KE, Oster-Jorgensen E, Krogdahl A, Hegedus L. Recurrent pregnancy-related upper airway obstruction caused by intratracheal ectopic thyroid tissue. Thyroid. 1999. 9:955–958.8. Muysomes F, Boedts M, Clayes D. Intratracheal ectopic thyroid tissue mass. Chest. 1993. 112:1684–1685.9. Freeman MS. Intratracheal goiter. Ohio Med. 1957. 53:1416–1417.10. Al-Hajjaj MS. Ectopic intratracheal thyroid presenting as bronchial asthma. Respiration. 1991. 58:329–331.11. Shankar P, Kilvert A, Fox C. Changing thyroid status related to pregnancy. Postgrad Med. 2001. 77:591–592.12. Fantz CR, Dagogo S, Ladenson JH, Gronowski AM. Thyroid function during pregnancy. Clin Chem. 1999. 45:2250–2258.13. Donegan JO, Wood MD. Intratracheal thyroid-familial occurrence. Laryngoscope. 1985. 95:6–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mediastinal Ectopic Thyroid Cyst Inducing Severe Airway Compression
- Unexpected Difficult Intubation due to Lingual Thyroid: A case report
- A Case of Neonatal Dual Ectopic Thyroid Glands with Congenital Hypothyroidism
- Adenomatous Hyperplasia Arising from Dual Ectopic Thyroid
- Two Cases of Lingual Thyroid
