Concurrent Renal Angiomyolipoma and Renal Cell Carcinoma: Report of Two Cases
- Affiliations
-
- 1Department of Radiology, Anam Hospital, College of Medicine, Korea University, Seoul, Korea. urorad@gmail.com
- 2Department of Pathology, Anam Hospital, College of Medicine, Korea University, Seoul, Korea.
- KMID: 2098004
- DOI: http://doi.org/10.3348/jksr.2014.71.4.186
Abstract
- Concurrent renal cell carcinoma (RCC) and angiomyolipoma (AML) is a very rare condition, especially in patients without underlying tuberous sclerosis. We present three patients with concurrent RCC and AML in the ipsilateral kidney. Concurrent RCC is difficult to differentiate radiologically from a non-fatty component of an AML because they share several imaging findings. However, several noticeable radiologic features are helpful in the diagnosis of suspected cases. This report of two cases highlights the radiologic features that distinguish RCC from non-fatty components of AML.
MeSH Terms
Figure
-
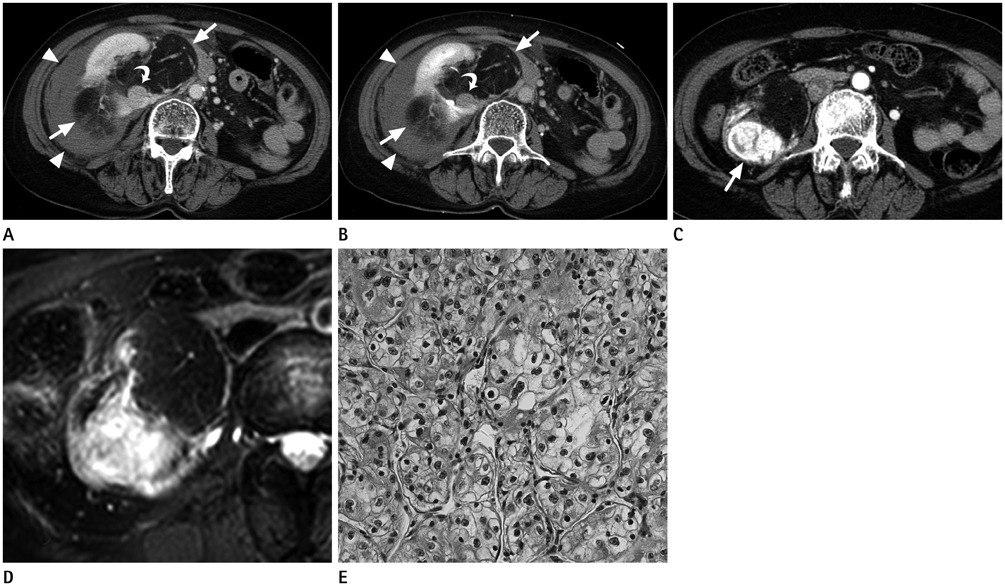
Fig. 1 Initial axial CT images of a 65-year-old female patient reveal a 20.0 × 15.8 × 10.1 cm lobulated contoured fatty mass (arrows) in the right kidney and hyperdense fluid collection (arrowheads) in the right perinephric space. Additionally, a 1.9-cm well-defined mass (curved arrow) adjacent to the inferior aspect of the fatty mass is identified. The enhancing mass shows contrast enhancement on the corticomedullary phase (A) and delayed wash-out on the excretory phase (B). Follow-up axial CT images on the corticomedullary phase after 55 months (C) demonstrates gradual growth of the enhancing mass (arrow) throughout the entire follow-up period. Multi Shot Turbo Spin Echo T2-weighted (repetition time/echo time = 1641/70 ms) spectral presaturation inversion recovery fat-suppression MRI (D) shows hyperintensity of the enhancing mass. Photomicrograph of the mass (E) shows a typical alveolar architectural pattern separated by thin-walled blood vessels, suggesting clear cell type renal cell carcinoma. The tumor cells have distinct cell borders and optically clear or eosinophilic granular cytoplasm (H&E, × 400).

Fig. 2 A coronal CT image of a 45-year-old male patient (A) reveals a 3.7-cm well-defined mass (arrow) and a 4.0-cm well-defined mass (curved arrow) in the right kidney upper pole and lower pole, respectively. The upper pole mass (arrow) shows strong heterogeneous enhancement on the corticomedullary phase (B).
Reference
-
1. Aron M, Aydin H, Sercia L, Magi-Galluzzi C, Zhou M. Renal cell carcinomas with intratumoral fat and concomitant angiomyolipoma: potential pitfalls in staging and diagnosis. Am J Clin Pathol. 2010; 134:807–812.2. Gutierrez OH, Burgener FA, Schwartz S. Coincident renal cell carcinoma and renal angiomyolipoma in tuberous sclerosis. AJR Am J Roentgenol. 1979; 132:848–850.3. Kato H TH, Furuse S, Sakata K, Morita T, Tokue A. Coincident renal cell carcinoma and renal angiomyolipoma in tuberous sclerosis: a case report. Rinsho Hoshasen. 2002; 47:582–586.4. Ueda J, Kobayashi Y, Itoh H, Itatani H. Angiomyolipoma and renal cell carcinoma occurring in same kidney: CT evaluation. J Comput Assist Tomogr. 1987; 11:340–341.5. Pierorazio PM, Hyams ES, Tsai S, Feng Z, Trock BJ, Mullins JK, et al. Multiphasic enhancement patterns of small renal masses (≤4 cm) on preoperative computed tomography: utility for distinguishing subtypes of renal cell carcinoma, angiomyolipoma, and oncocytoma. Urology. 2013; 81:1265–1271.6. Jimenez RE, Eble JN, Reuter VE, Epstein JI, Folpe AL, de Peralta-Venturina M, et al. Concurrent angiomyolipoma and renal cell neoplasia: a study of 36 cases. Mod Pathol. 2001; 14:157–163.7. Mai KT, Perkins DG, Robertson S, Thomas J, Morrash C, Collins JP. Composite renal cell carcinoma and angiomyolipoma: a study of the histogenetic relationship of the two lesions. Pathol Int. 1999; 49:1–8.8. Yamamoto S, Nakamura K, Kawanami S, Aoki T, Watanabe H, Nakata H. Renal angiomyolipoma: evolutional changes of its internal structure on CT. Abdom Imaging. 2000; 25:651–654.9. Lee JY, Kim CK, Choi D, Park BK. Volume doubling time and growth rate of renal cell carcinoma determined by helical CT: a single-institution experience. Eur Radiol. 2008; 18:731–737.10. Vargas HA, Chaim J, Lefkowitz RA, Lakhman Y, Zheng J, Moskowitz CS, et al. Renal cortical tumors: use of multiphasic contrast-enhanced MR imaging to differentiate benign and malignant histologic subtypes. Radiology. 2012; 264:779–788.11. Kim JK, Park SY, Shon JH, Cho KS. Angiomyolipoma with minimal fat: differentiation from renal cell carcinoma at biphasic helical CT. Radiology. 2004; 230:677–684.12. Pedrosa I, Sun MR, Spencer M, Genega EM, Olumi AF, Dewolf WC, et al. MR imaging of renal masses: correlation with findings at surgery and pathologic analysis. Radiographics. 2008; 28:985–1003.13. Taouli B, Thakur RK, Mannelli L, Babb JS, Kim S, Hecht EM, et al. Renal lesions: characterization with diffusion-weighted imaging versus contrast-enhanced MR imaging. Radiology. 2009; 251:398–407.14. Zhang YL, Yu BL, Ren J, Qu K, Wang K, Qiang YQ, et al. EADC Values in Diagnosis of Renal Lesions by 3.0 T Diffusion-Weighted Magnetic Resonance Imaging: Compared with the ADC Values. Appl Magn Reson. 2013; 44:349–363.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coincidental occurrence of renal cell carcinoma and angiomyolipoma in the same kidney : a case report
- Multiloculated Cystic Type Renal Epithelioid Angiomyolipoma Mimicking Renal Cell Carcinoma: A Case Report
- Renal Angiomyolipoma: Report of 6 cases and Review of the Literature
- A Case of Renal Angiomyolipoma
- RE: Distinguishing between Renal Cell Carcinoma and Fat Poor Angiomyolipoma in Diffusion-Weighted Imaging
