Percutaneous N-Butyl Cyanoacrylate Embolization of a Pancreatic Pseudoaneurysm after Failed Attempts of Transcatheter Embolization
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, Seoul National University Medical Research Center, and Clinical Research Institute, Seoul National University Hospital, Seoul, Korea. angiointerventio
- KMID: 2098001
- DOI: http://doi.org/10.3348/jksr.2014.71.4.173
Abstract
- One common complication after major pancreatic surgery is bleeding. Herein we describe a case of pancreatic pseudoaneurysm which developed after pylorous preserving pancreaticoduodenectomy for common bile duct cancer. Three attempts of transcatheter embolization failed since feeders to the pseudoaneurysm had unfavorable anatomy. Direct percutaneous N-butyl cyanoacrylate injection was performed under fluoroscopy-guidance and the pseudoaneurysm was successfully treated. Percutaneous fluoroscopy-guided direct N-butyl cyanoacrylate injection may be a useful alternative when selective transcatheter embolization fails or is technically challenging.
MeSH Terms
Figure
-
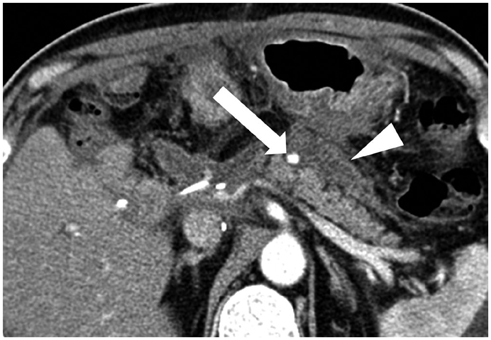
Fig. 1 The contrast-enhanced abdominal CT scan (arterial phase) taken 16 days after pylorous preserving pancreaticoduodenectomy for common bile duct cancer shows a 6.2-mm pseudoaneurysm (arrow). The extent of hematoma between the pancreas and the stomach (arrowhead) was slightly decreased after insertion of a drainage catheter (not shown).
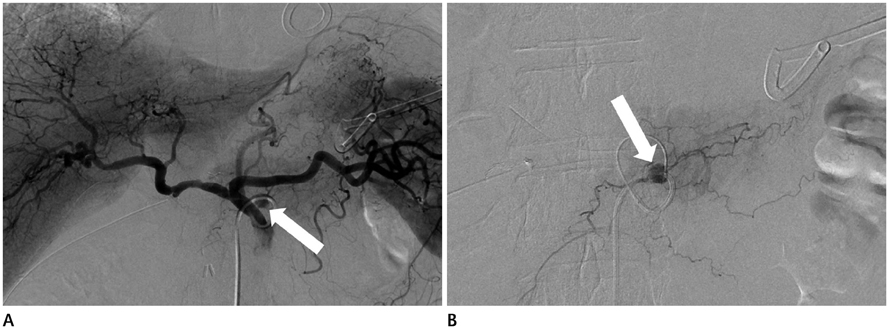
Fig. 2 Angiography was performed 16 days after pylorous preserving pancreaticoduodenectomy. A. Celiac angiography shows a pseudoaneurysm at the dorsal pancreatic artery (arrow). B. Selective angiography of the dorsal pancreatic artery demonstrates the pseudoaneurysm (arrow) connected with several small pancreatic branches.
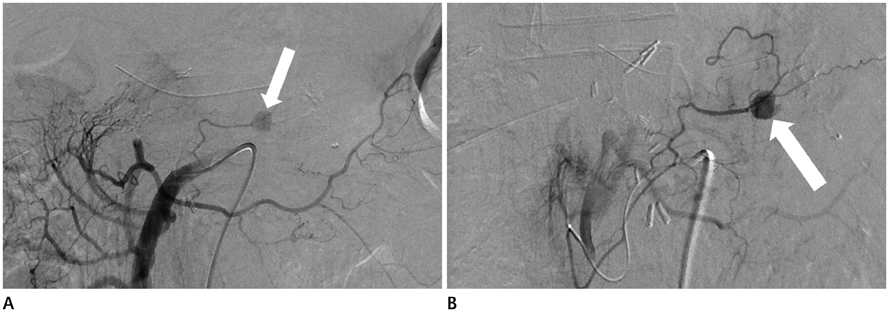
Fig. 3 The 3rd trial of transcatheter embolization was performed 24 days after pylorous preserving pancreaticoduodenectomy. A. Superior mesenteric angiography at the second attempt reveals a feeding vessel to the pseudoaneurysm (arrow). B. Selective angiography of the pancreaticoduodenal artery from the superior mesenteric artery shows that the feeding vessel of the pseudoaneurysm (arrow) is very tortuous and angulated.
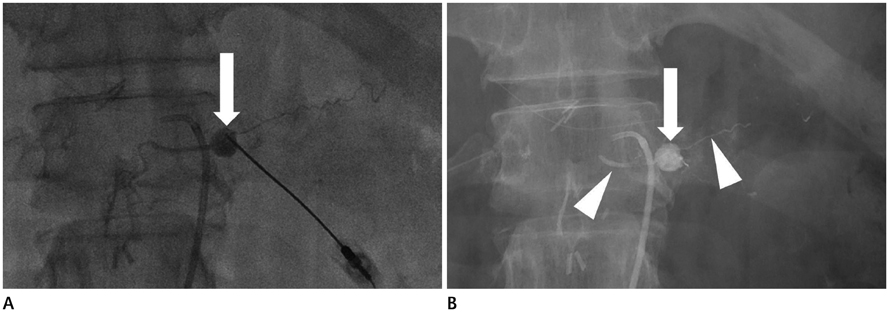
Fig. 4 Percutaneous fluoroscopy-guided direct N-butyl cyanoacrylate injection was performed 24 days after pylorous preserving pancreaticoduodenectomy. A. Direct percutaneous puncture of the pseudoaneurysm (arrow) was carried out under fluoroscopic guidance. B. The post-procedural fluoroscopic image shows compact filling of N-butyl cyanoacrylate in the pseudoaneurysm (arrow) as well as vessels (arrowheads) connected with the pseudoaneurysm.
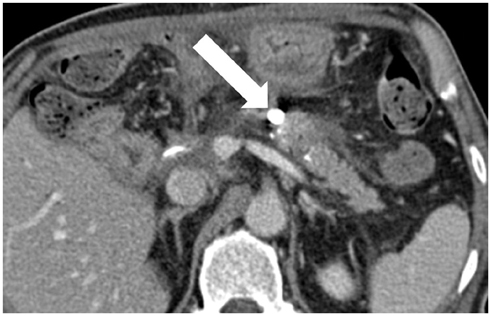
Fig. 5 The follow-up contrast-enhanced CT scan taken seven days after the embolization demonstrates compact filling of the pseudoaneurysm (arrow) with the NBCA and iodized oil mixture. CT scan 18 months after the procedure showed no recurrence of pseudoaneurysm (not shown).
Reference
-
1. Ding X, Zhu J, Zhu M, Li C, Jian W, Jiang J, et al. Therapeutic management of hemorrhage from visceral artery pseudoaneurysms after pancreatic surgery. J Gastrointest Surg. 2011; 15:1417–1425.2. Bergert H, Dobrowolski F, Caffier S, Bloomenthal A, Hinterseher I, Saeger HD. Prevalence and treatment of bleeding complications in chronic pancreatitis. Langenbecks Arch Surg. 2004; 389:504–510.3. Schäfer M, Heinrich S, Pfammatter T, Clavien PA. Management of delayed major visceral arterial bleeding after pancreatic surgery. HPB (Oxford). 2011; 13:132–138.4. Otah E, Cushin BJ, Rozenblit GN, Neff R, Otah KE, Cooperman AM. Visceral artery pseudoaneurysms following pancreatoduodenectomy. Arch Surg. 2002; 137:55–59.5. Vyas S, Ahuja CK, Yadav TD, Khandelwal N. Emergency ultrasound-guided percutaneous embolization of post-traumatic bleeding hepatic artery pseudoaneurysms. Minim Invasive Ther Allied Technol. 2012; 21:372–376.6. Cope C, Zeit R. Coagulation of aneurysms by direct percutaneous thrombin injection. AJR Am J Roentgenol. 1986; 147:383–387.7. Araoz PA, Andrews JC. Direct percutaneous embolization of visceral artery aneurysms: techniques and pitfalls. J Vasc Interv Radiol. 2000; 11:1195–1200.8. Ghassemi A, Javit D, Dillon EH. Thrombin injection of a pancreaticoduodenal artery pseudoaneurysm after failed attempts at transcatheter embolization. J Vasc Surg. 2006; 43:618–622.9. Aytekin C, Firat A, Yildirim E, Kirbas I, Boyvat F. Ultrasound-guided glue injection as alternative treatment of femoral pseudoaneurysms. Cardiovasc Intervent Radiol. 2004; 27:612–615.10. Gulati GS, Gulati MS, Makharia G, Hatimota P, Saikia N, Paul SB, et al. Percutaneous glue embolization of a visceral artery pseudoaneurysm in a case of sickle cell anemia. Cardiovasc Intervent Radiol. 2006; 29:665–668.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posttraumatic Pseudoaneurysm in Scalp Treated by Direct Puncture Embolization Using N-Butyl-2-Cyanoacrylate: a Case Report
- Transcatheter Arterial Embolization with N-Butyl Cyanoacrylate for Profunda Femoris Artery Pseudoaneurysms Caused by Femur Shaft Fractures: Two Case Reports
- Transcatheter Arterial Embolization of Cystic Artery Pseudoaneurysm in Acalculous Cholecystitis: A Case Report
- Multiple Cerebral Infarction after Injection of N-Butyl-2-Cyanoacrylate for Gastric Variceal Bleeding
- Successful Transcatheter Emvolization of Pseudoaneurysm Caused by Pancreatitis
