Segmental Adenomyomatosis of Gallbladder: CT Assessment of the Patterns of Cholecystolithiasis
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Yonsei University College of Medicine, Korea. yjsrad97@yuhs.ac
- KMID: 2097947
- DOI: http://doi.org/10.3348/jksr.2011.64.3.253
Abstract
- PURPOSE
To clarify the relationship between the pattern of cholecystolithiasis and the gross features of segmental adenomyomatosis of the gallbladder.
MATERIALS AND METHODS
Fifty-five consecutive patients with segmental adenomyomatosis with calcified gallbladder stones defined on CT were retrospectively analyzed in terms of (i) stone location (fundal vs. neck compartment) and (ii) size of the largest stone as a function of the extent of segmental mural thickening (type A, limited at the narrow segment; type B, partially extended in the fundal direction; type C, involving the entire fundal compartment). The extent of segmental mural thickening in patients with cholecystolithiasis was compared with a control group (n = 48) lacking stones.
RESULTS
Stones were found more frequently in the fundal compartment in 48 patients compared to the neck compartment in 12 patients (p<0.001). The mean size of the largest stone in type C (5.4 +/- 4.9 mm) was larger than in type A (2.3 +/- 2.2 mm) (p=0.033). In patients with cholecystolithiasis, type C segmental thickening was predominant (69%) compared to the control group (42%) (p=0.012).
CONCLUSION
In addition to a higher prevalence of stones, a wide extent of mural thickening combined with large stone size in the fundal compartment suggests the contribution of segmental adenomyomatosis to stone formation and chronic inflammation.
MeSH Terms
Figure
-
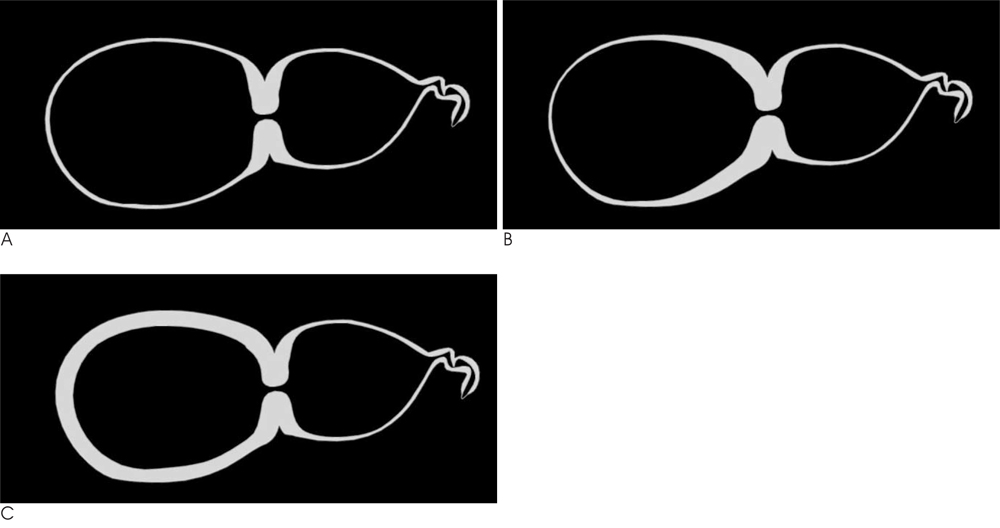
Fig. 1 Schematic drawing of the different types of segmental adenomyomatosis of the gallbladder. A. Type A represents a mural thickening limited to the narrow segment. B. Type B represents a mural thickening partially extended in the fundal direction C. Type C represents a mural thickening involving the entire fundal compartment of the gallbladder.
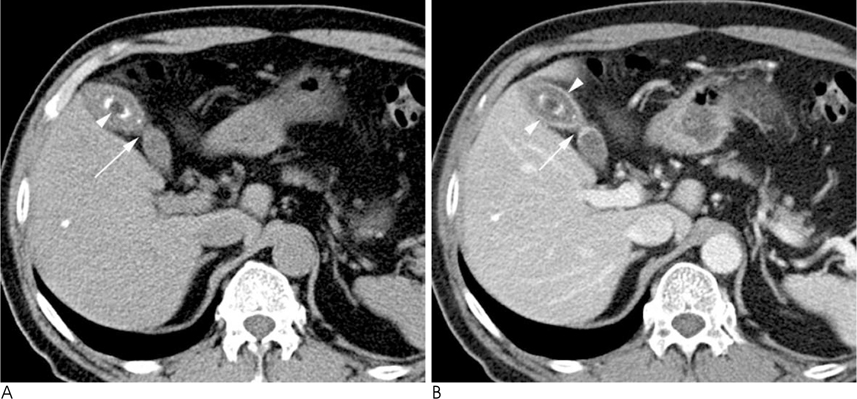
Fig. 2 A 64-year-old man with segmental adenomyomatosis with a calcified GB stone and mural thickening involving the entire fundal compartment (type C). A. This precontrast axial CT image shows focal luminal narrowing of GB (arrow) with a 1.8 cm calcified stone in the fundal compartment (arrowheads). B. Post-contrast axial CT image showing a diffusely thickened wall with abnormal contrast enhancement including the entire fundal compartment (arrowheads) and the narrowing segment (arrow).

Fig. 3 A 31-year-old man with segmental adenomyomatosis with multiple calcified sandy stones in the fundal compartment and mural thickening partially extended in the fundal direction (type B). A. Precontrast axial CT image showing innumerable calcified sandy stones (arrow) in the fundal portion of the GB. B, C. Post-contrast axial (B) and coronal (C) CT images showing segmental luminal narrowing (arrow) and mural thickening partially extended in the fundal direction (arrowheads).

Fig. 4 A 40-year-old woman with segmental adenomyomatosis without cholecystolithiasis showing the mural thickening limited to the narrowing segment (type A). A. This postcontrast axial CT image shows an en face view of the circumferentially thickened wall with luminal narrowing (arrow) at the body portion of the GB. B. Post-contrast coronal CT image showing segmental luminal narrowing (arrow) with no abnormal mural thickening in the remaining GB wall and no intraluminal calcified stone density.
Reference
-
1. Colquhoun J. Adenomyomatosis of the gall-bladder (intramural diverticulosis). Br J Radiol. 1961; 34:101–112.2. Jutras JA. Hyperplastic cholecystoses; Hickey lecture, 1960. Am J Roentgenol Radium Ther Nucl Med. 1960; 83:795–827.3. Kasahara Y, Sonobe N, Tomiyoshi H, Imano M, Nakatani M, Urata T, et al. Adenomyomatosis of the gallbladder: a clinical survey of 30 surgically treated patients. Nippon Geka Hokan. 1992; 61:190–198.4. Tanno S, Obara T, Maguchi H, Fujii T, Mizukami Y, Shudo R, et al. Association between anomalous pancreaticobiliary ductal union and adenomyomatosis of the gall-bladder. J Gastroenterol Hepatol. 1998; 13:175–180.5. Kurihara K, Mizuseki K, Ninomiya T, Shoji I, Kajiwara S. Carcinoma of the gall-bladder arising in adenomyomatosis. Acta Pathol Jpn. 1993; 43:82–85.6. Nishimura A, Shirai Y, Hatakeyama K. Segmental adenomyomatosis of the gallbladder predisposes to cholecystolithiasis. J Hepatobiliary Pancreat Surg. 2004; 11:342–347.7. Ootani T, Shirai Y, Tsukada K, Muto T. Relationship between gallbladder carcinoma and the segmental type of adenomyomatosis of the gallbladder. Cancer. 1992; 69:2647–2652.8. Klose KC, Persigehl M, Biesterfeld S, Gunther RW. Adenomyomatosis of the gallbladder in CT. Radiologe. 1991; 31:73–81.9. Chao C, Hsiao HC, Wu CS, Wang KC. Computed tomographic finding in adenomyomatosis of the gallbladder. J Formos Med Assoc. 1992; 91:467–469.10. Kim MJ, Oh YT, Park YN, Chung JB, Kim DJ, Chung JJ, et al. Gallbladder adenomyomatosis: findings on MRI. Abdom Imaging. 1999; 24:410–413.11. Nussle K, Brambs HJ, Rieber A. Adenomyomatosis of the gallbladder: ultrasound findings. Rontgenpraxis. 1998; 51:155–158.12. Gore RM, Levin MS. Textbook of Gastrointestinal Radiology. 3rd ed. Philadelphia: Saunders/Elsevier;2008. p. 1446–1447.13. Vilkin A, Nudelman I, Morgenstern S, Geller A, Bar Dayan Y, Levi Z, et al. Gallbladder inflammation is associated with increase in mucin expression and pigmented stone formation. Dig Dis Sci. 2007; 52:1613–1620.14. Domeyer PJ, Sergentanis TN, Zagouri F, Tzilalis B, Mouzakioti E, Parasi A, et al. Chronic cholecystitis in elderly patients. Correlation of the severity of inflammation with the number and size of the stones. In Vivo. 2008; 22:269–272.15. Hsing AW, Gao YT, Han TQ, Rashid A, Sakoda LC, Wang BS, et al. Gallstones and the risk of biliary tract cancer: a populationbased study in China. Br J Cancer. 2007; 97:1577–1582.16. Owen CC, Bilhartz LE. Gallbladder polyps, cholesterolosis, adenomyomatosis, and acute acalculous cholecystitis. Semin Gastrointest Dis. 2003; 14:178–188.17. Yang HL, Li ZZ, Sun YG. Reliability of ultrasonography in diagnosis of biliary lithiasis. Chin Med J (Engl). 1990; 103:638–641.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenocarcinoma Arising in Segmental Adenomyomatosis of the Gallbladder: A Case Report
- Focal Thickening at the Fundus of the Gallbladder: Computed Tomography Differentiation of Fundal Type Adenomyomatosis and Localized Chronic Cholecystitis
- Heterotopic pancreas of the gallbladder associated with segmental adenomyomatosis of the gallbladder
- Localized Adenomyomatosis of Gallbladder Mimicking Advanced Hepatic Flexure Colon Cancer: A Case Report
- Report of a Case of Adenomyomatosis of Gallbladder
