Pneumomediastinum on Multidetector CT: The Radiologic Signs and Underlying Disorders
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Chunan Hospital, Korea. ytokim@scha.ac.kr
- KMID: 2097932
- DOI: http://doi.org/10.3348/jksr.2011.64.2.157
Abstract
- We can see the typical signs of pneumomediastinum on chest radiography and we can also see them on the multiplanar reformatted (MPR) image of multidetector CT (MDCT). MDCT can help to understand the anatomical feature of these signs and differentiate pneumomediastinum from pneumothorax, pneumopericardium and the Mach band effect. MDCT shows the peribronchovascular air, which reveals the Macklin effect, and it can also evaluate the underlying disorders that cause pneumomediastinum. The purpose of this pictorial essay is to inform physicians about the mechanism and anatomical features of pneumomediastinum, and to help them understand the imaging findings and underlying disorders of pneumomediastinum as seen on MDCT.
Figure
-
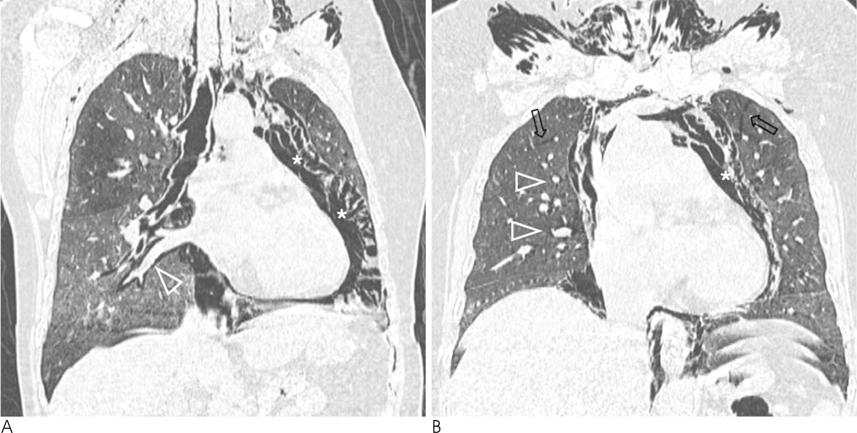
Fig. 1 Pneumomediastinum from extensive paraquat induced lung injury in a 44-year-old woman. She expired the next day after CT scanning. A. Reformatted oblique coronal image shows interstitial air collection (open arrowhead) along peribronchovascular bundle in the right lower lobe. Extensive ground-glass opacities in both lungs are compatible with CT findings of extensive paraquat-induced lung injury. B. Reformatted coronal image shows intraparenchymal interstitial emphysema (open arrows) in both upper lobes, and interstitial emphysema along peribronchovascular bundles (open arrowheads) in the right lung. Also seen extensive pneumomediastinum (*) with irregular linear structures by connective tissue.

Fig. 2 Pneumomediastinum from endoscopic submucosal dissection of esophageal cancer in a 73-year-old man. A. Chest radiograph shows multiple linear radiolucencies in superior mediastinum, mediastinal air (*) in right sided mediastinum, and air outlining aortic arch (open arrow). Also note a tubular structure (arrow), which represents air surrounding right brachiocephalic vein, and V shaped air shadow (open arrowhead) at the confluence of brachiocephalic veins. B. Lateral radiograph shows broad band of mediastinal air (arrowheads) separating anterior pericardium from sternum, and air outlining aortic arch (open arrow).
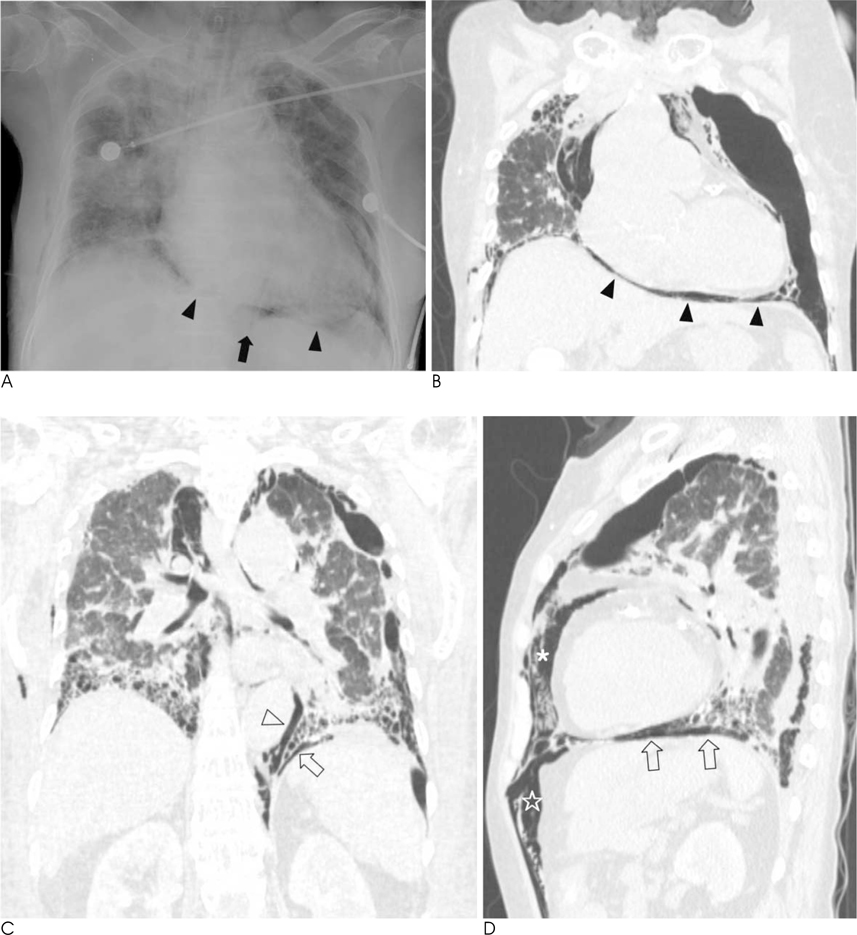
Fig. 3 Pneumomediastinum from necrotizing fascitis of neck in a 75-year-old woman. A. Chest radiograph shows thin band of air collection between heart and diaphragm (arrowheads), known as continuous diaphragm sign. Also note Naclerio's V sign (arrow) at the medial portion of left diaphragm. B. Reformatted coronal image shows air collection (arrowheads) between pericardium and diaphragm. C. On reformatted coronal image, Naclerio's V sign consists of vertical extrapleural air outlining descending aorta (open arrowhead) and oblique extrapleural air between parietal pleura and left hemidiaphragm (open arrow). D. Reformatted sagittal image shows mediastinal air (*) extending to anterior extraperitoneal space (☆). Also note extrapleural air collection (open arrows) between parietal pleura and diaphragm.

Fig. 4 Pneumomediastinum from spontaneous cause in a 27-year-old man. A, B. Chest radiograph (A) and refomatted coronal image (B) show visualization of both sides of bronchial wall (open arrowheads), known as double bronchial wall sign. Also note extrapleural extension (open arrows) of pneumomediastinum in the left lung apex. At the left lung apex, extrapleural extension (open arrows) from mediastinal air does not form smooth arcs with visible webs of connective tissue outside pleural line, which helps distinguish extrapleural extension of pneumomediastinum from pneumothorax.

Fig. 5 Pneumomediastinum from motor vehicle accident in a 67-year-old man. Axial image shows mediastinal air extending to anterior extrapleural space (*). Also note subcutaneous emphysema in both chest wall.

Fig. 6 Spontaneous pneumomediastinum with extrapleural air extention in a 51-year-old woman. She complained of severe cough, sputum and dypnea. A. Axial CT image shows multiseptated air collectios (*) in the medial portion of the left upper lobe, mimicking bullae, and pneumomediastinum (arrow heads). Also note underlying bronchectasis and sequelea of pulmonary tuberculosis in the both lungs. B. Axial CT scan 1 year later shows spontaneous resolution of multiseptated air collections. It suggestive of unusual manifestation of extrapleural extension from pneumomediastinum.

Fig. 7 Pneumomediastinum caused by transverse colon perforation in a 67-year-old woman A, B. Abdominal radiograph (A) and reformatted coronal image (B) show the retroperitoneal air collection (arrow heads) outlining the kidney, extending to mediastinum (arrow). Also note pneumoperitoneum.
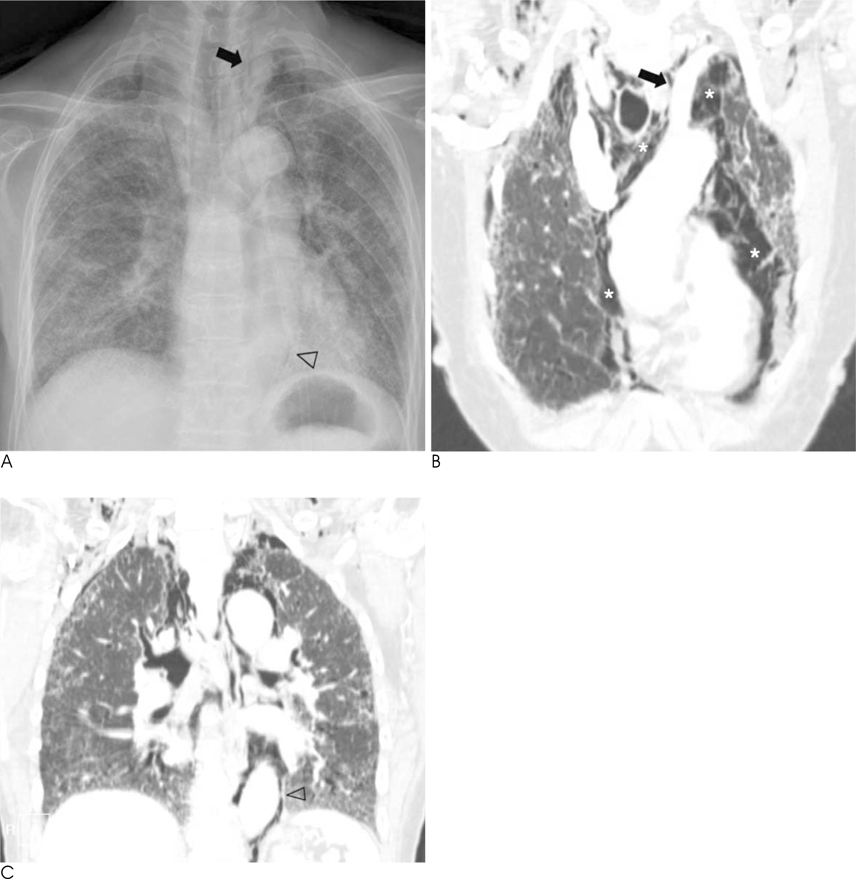
Fig. 8 Pneumomediastinum from idiopathic pulmonary fibrosis in a 84-year-old woman. A. Chest radiograph shows tubular structure (arrow) by mediastinal air surrounding left subclavian artery, and extrapleural sign (open arrowhead) outside the descending aorta. B. Reformatted oblique coronal image shows mediastinal air (arrow) surrounding the left subclavian artery. Also note extensive mediastinal air (*) with irregular linear structures by connective tissue. Note fibrosis and traction bronchiectasis in subpleural area of the both lungs. C. Reformatted coronal image shows extrapleural sign (open arrowhead) by air collection outlining descending aorta.
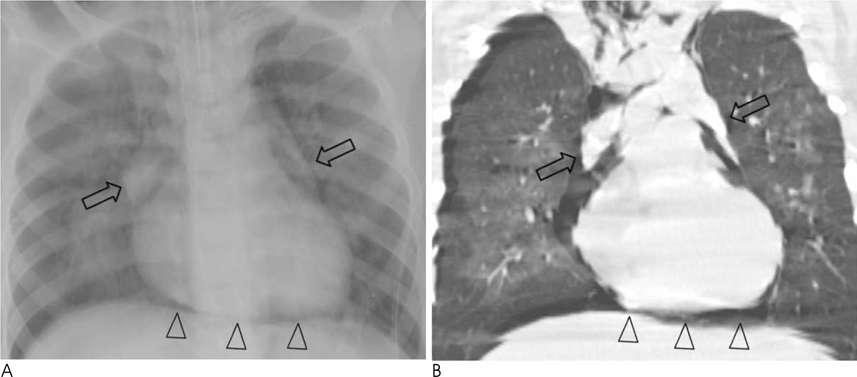
Fig. 9 Pneumomediastinum from pneumonia in a 8-year-old boy. A, B. Chest radiograph (A) and reformatted coronal image (B) show pneumomediastinum elevating thymic lobes (arrows), known as thymic sail sign. Also note continuous diaphragm sign (arrowheads), and subcutaneous emphysema of neck and upper chest wall.
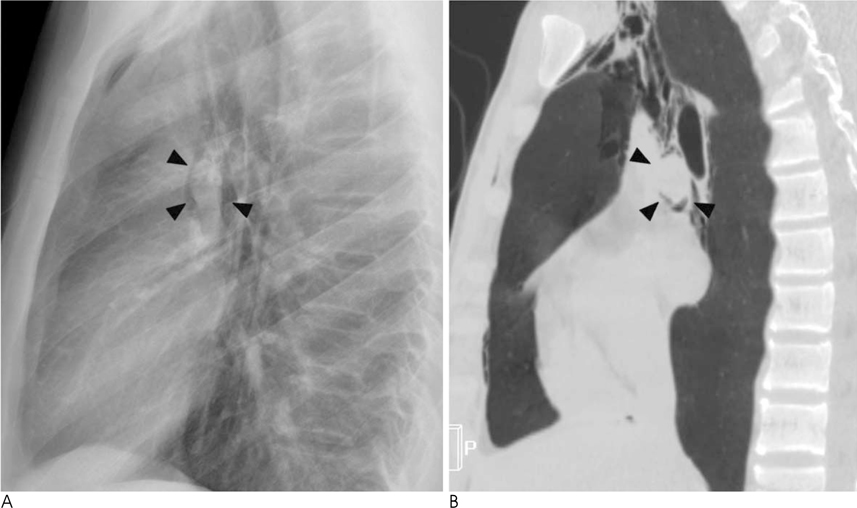
Fig. 10 Spontaneous pneumomediastinum in a 15-year-old boy. A, B. Lateral chest radiograph (A) and reformatted sagittal image (B) show a air shadow (arrow heads) around the left pulmonary artery, known as the ring-around-the-artery sign.
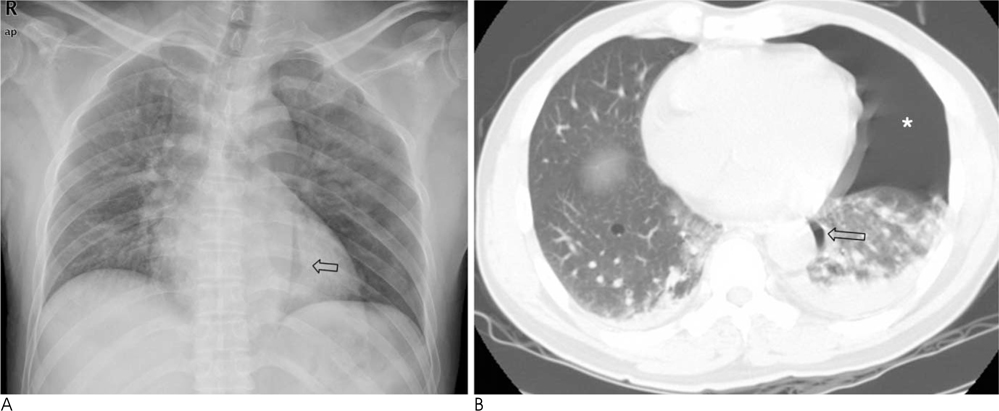
Fig. 11 Medial pneumothorax in a 43-year-old man A. Supine chest radiograph shows localized air collection (open arrow) outside descending thoracic aorta. It simulates the extrapleural sign of pneumomediastinum. B. Axial CT scan with lung setting shows localized pneumothorax (open arrow) lateral to descending thoracic aorta. Also note pneumothorax (*) in the nondependent portion of the left hemithorax.

Fig. 12 Pneumopericardium from stab injury in a 40-year-old man. Chest radiograph shows pericardial air collection around heart, which is not extend above aortic arch.
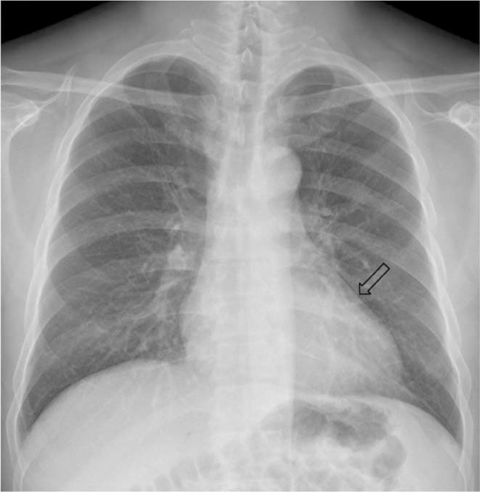
Fig. 13 Mach band effect in a 48-year-old man. Chest radiograph shows radiolucent line (open arrow) outlining left cardiac border.

Fig. 14 Pneumomediastinum from bronchial injury caused by motor vehicle accident in a 10-year-old boy. Axial CT scan with lung setting after chest thoracotomy shows poorly delineated posterior wall of left main bronchus (arrowhead). Also note delineated air, subcutaneous emphysema, and bilateral extensive consolidations.
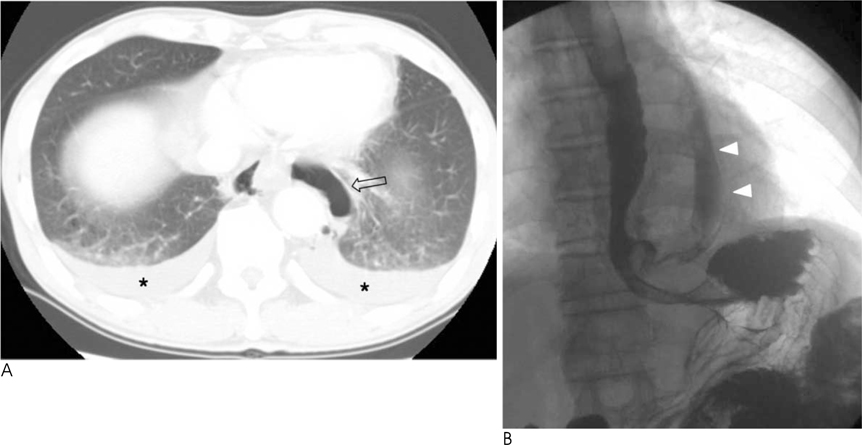
Fig. 15 Pneumomediastinum from spontaneous esophageal perforation in a 77-year-old man. A. Axial CT scan with lung setting shows air collection around distal esophagus (open arrow), and bilateral pleural effusion (*). B. Esophagogram shows the leakage of contrast media (arrowheads) from distal esophagus.

Fig. 16 Pneumomediastinum from infectious mediastinitis in a 34-year-old man. Axial CT scan shows fluid collection with dirty air shadows in the anterior mediastinum.
Reference
-
1. Macia I, Moya J, Ramos R, Morera R, Escobar I, Saumench J, et al. Spontaneous pneumomediastinum: 41 cases. Eur J Cardiothorac Surg. 2007; 31:1110–1114.2. Bejvan SM, Godwin JD. Pneumomediastinum: old signs and new signs. AJR Am J Roentgenol. 1996; 166:1041–1048.3. Macklin CC. Transport of air along sheaths of pulmonic blood vessels from alveoli to mediastinum: clinical implications. Arch Intern Med. 1939; 64:913–926.4. Jeon KN, Bae K, Yoo JJ, Jung SH, Kang DS. Pneumothorax, Pneumomediastinum and Pneumopericardium: A Pictorial Review. J Korean Radiol Soc. 2004; 50:255–262.5. Bullaro FM, Bartoletti SC. Spontaneous pneumomediastinum in children: a literature review. Pediatr Emerg Care. 2007; 23:28–30.6. Hartley C, Morritt GN. Bronchial rupture secondary to blunt chest trauma. Thorax. 1993; 48:183–184.7. Fujiwara T. Pneumomediastinum in pulmonary fibrosis. Detection by computed tomography. Chest. 1993; 104:44–46.8. Sittipunt C. Paraquat poisoning. Respir Care. 2005; 50:383–385.9. Pierce TB, Razzuk MA, Razzuk LM, Luterman DL, Sutker WL. Acute mediastinitis. Proc (Bayl Univ Med Cent). 2000; 13:31–33.10. Marty-Ane CH, Alauzen M, Alric P, Serres-Cousine O, Mary H. Descending necrotizing mediastinitis. Advantage of mediastinal drainage with thoracotomy. J Thorac Cardiovasc Surg. 1994; 107:55–61.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiseptated Cystic Pneumomediastinum in a Term Newborn: Cystic and Bubbly Lesion on Chest X-ray
- A Case of Cystic Pneumomediastinum with Thymic Hyperplasia in a Newborn
- Spontaneous Pneumomediastinum on CT: Related Condition and its Clinical Significance
- Pneumothorax, Pneumomediastinum and Pneumopericardium: A Pictorial Review
- Multidetector Row Computed Tomography: 'Principles and Clinical Applications'
