The First Report on Evaluating the Thoracic Radiology of the Medical Institutions for Pneumoconiosis in Korea
- Affiliations
-
- 1Occupational Lung Diseases Institute, COMWEL, Korea. atomlwj@kmedi.or.kr
- 2Department of Radiology, Soonchunhyang University Bucheon Hospital, Korea.
- 3Department of Radiology, Chungbuk University Hospital, Korea.
- 4Center for Occupational Disease Research, OSHRI, Korea.
- KMID: 2097913
- DOI: http://doi.org/10.3348/jksr.2010.63.5.431
Abstract
- PURPOSE
The pnuemoconiotic findings on chest radiograph for pneumoconiosis are affected by the technique, the equipment and the reading environment. We report here on the results of evaluating the thoracic radiology of the Medical Institutions for Pneumoconiosis (MIPs).
MATERIALS AND METHODS
For the first time, we visited the MIPs to evaluate the thoracic radiography that is used to treat patients with pneumoconiotic complications, and this included evaluating the equipment and the technical parameters for thoracic radiography, the computed tomography, the education for quality assurance health care and the reading environment. We used the guideline published by the Occupational Safety and Health Research Institute (OSHRI). Ten images were randomly picked from the MIPs for evaluating the image quality, and then these were rated by two experienced chest radiologists for pneumoconiosis according to thecriteria of the OSHRI.
RESULTS
Of the 33 institutions, the failed group (mean<60) scored 36.4% for radiological technique (RT),30.3% for image quality (IQ) and 21.2% for the reading environment (RE). There were statistically significantly differences between the passed and failed groups for RT (75.8 +/- 9.1 vs. 40.8 +/- 13.6, p<0.001), for IQ (68.3 +/- 5.8 vs. 47.8 +/- 9.4, p<0.001) and for RE (78.3 +/- 15.8 vs. 18.3 +/- 21.9, p<0.001). The group that received education was significantly higher for the RT (68.7 vs. 53.2, p=0.032), the IQ (65.3 vs. 56.6, p=0.039) and the RE(76.2 vs. 47.0, p=0.005) than that for the group that didn't receive education.
CONCLUSION
The MIPs need surveillance and education for improving the quality assurance health care in thoracic radiography for treating patients with pneumoconiosis and who have complications.
MeSH Terms
Figure
-
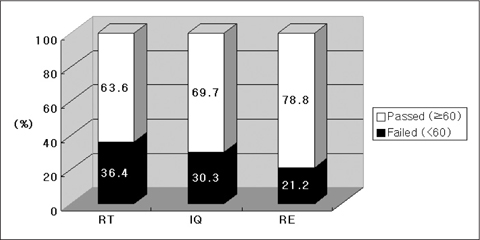
Fig. 1 Graph shows that frequency between passed and failed groups in RT (Radiological technique), IQ (Image quality) and RE (Reading environment). Mean score of RT is statistically significantly higher in passed group than that in failed group (75.8 ± 9.1 vs. 40.8 ± 13.6, p<0.001). Mean score of IQ is statistically significantly higher in passed group than that in failed group (68.3 ± 5.8 vs. 47.8 ± 9.4, p<0.001). Mean score of RE is statistically significantly higher in passed group than that in failed group (78.3 ± 15.8 vs. 18.3 ± 21.9, p<0.001).
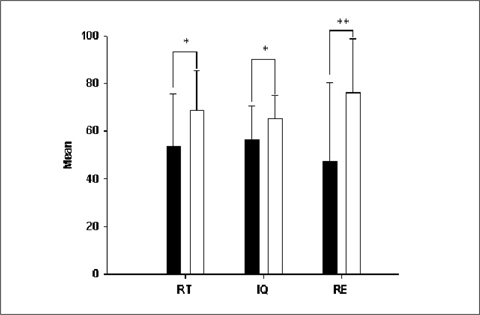
Fig. 2 Educated institutions showed significant high scores in RT (68.7 vs. 53.2, p=0.032), IQ (65.3 vs. 56.6, p=0.039) and RE (76.2 vs. 47.0, p=0.005) than uneducated institutions. (▪) uneducated institutions, (□) Educated institutions. * ; p<0.05, ** ; p<0.01

Fig. 3 This medical institution for pneumoconiosis was not using the grid. The score of RT and IQ were 28.6, 43.3, respectively.

Fig. 4 The chest image digitized from analog radiograph found that a defect of technical quality which was not completely shown at the chest wall and costophrenic angle of right side (IQ score=38.2).
Reference
-
1. Choi JI, Na DG, Kim HH, Shin YM, Ahn KJ, Lee JY. Quality Control of Medical Imaging. J Korean Radiol Soc. 2004; 50:317–331.2. Choi BS. Comparison of Radiological Methods for the Study and Diagnosis of Pneumoconiosis: Simple Radiography and Computed Tomography. Korean J Occup Environ Med. 1995; 7:390–424.3. Weill H. Diagnosis of asbestos-related disease. Chest. 1987; 91:802–803.4. Goodman LR, Wilson CR, Foley WD. Digital radiography of the chest: promises and problems. AJR Am J Roentgenol. 1988; 150:1241–1252.5. Wagner GR, Attfield MD, Parker JE. Chest radiography in dust-exposed miners: promise and problems, potential and imperfections. Occup Med. 1993; 8:127–141.6. J Radiol Sci Technol. 2010; 33:85–91.7. [Internet]. cited: July 10, 2008. Available from: http://oshri.kosha.or.kr/board?tc=RetrieveBoardViewCmd&boardType=A&contentId=208741&pageNum=1&urlCode=T1|Y|404|371|||||/board&tabId.8. Pham QT. Chest radiography in the diagnosis of pneumoconiosis. Int J Tuberc Lung Dis. 2001; 5:478–482.9. ILO. Guidelines for the use of ILO international classification of radiographs of pneumoconioses. Geneva: International Labour Office;1980.10. ILO. Guidelines for the use of ILO international classification of radiographs of pneumoconioses. Geneva: International Labour Office;2000.11. Park B, Sung DW. A Comparative Study of Image Quality and Radiation Dose with Changes in Tube Voltage and Current for a Digital Chest Radiography. J Korean Soc Radiol. 2010; 62:131–137.12. Woodard PK, Slone RM, Sagel SS, Fleishman MJ, Gutierrez FR, Reiker GG, et al. Detection of CT-proved pulmonary nodules: comparison of selenium-based digital and conventional screen-film chest radiographs. Radiology. 1998; 209:705–709.13. Bacher K, Smeets P, Vereecken L, De Hauwere A, Duyck P, De Man R, et al. Image quality and radiation dose on digital chest imaging: comparison of amorphous silicon and amorphous selenium flat-panel systems. AJR Am J Roentgenol. 2006; 187:630–637.14. Schaefer-Prokop C, Neitzel U, Venema HW, Uffmann M, Prokop M. Digital chest radiography: an update on modern technology, dose containment and control of image quality. Eur Radiol. 2008; 18:1818–1830.15. Choi BS. Factors affecting Reading Agreement of Pneumoconiotic Findings. Korean J Occup Environ Med. 1997; 9:614–627.16. Takashima Y, Suganuma N, Sakurazawa H, Itoh H, Hirano H, Shida H, et al. A flat-panel detector digital radiography and a storage phosphor computed radiography: screening for pneumoconiosis. J Occup Health. 2007; 49:39–45.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship of Image Quality and Radiation Dose for Chest Radiography in the Medical Institutions for Pneumoconiosis: A Comparison to the Korean Diagnostic Reference Level
- A Case of Caplan`s Syndrome with Pulmonary Tuberculosis
- Smoking Habit of Coal Workers' Pneumoconiosis Patients: Their Relationship to the Findings of Chest Radiographs
- Welder' Pneumoconiosis of Shipyard and related Factors
- Chest Radiological Changes after Cessation and Decrease of Exposure to Welding Fume in Shipyard Welders
