Childhood Brugada Syndrome in Two Korean Families
- Affiliations
-
- 1Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea. eunjbaek@snu.ac.kr
- 2Department of Laboratory Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Laboratory Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 2094076
- DOI: http://doi.org/10.4070/kcj.2010.40.3.143
Abstract
- Since the first descriptions of Brugada as a new clinical entity defined by sudden cardiac death in patients with typical electrocardiogram (ECG) patterns, Brugada syndrome (BS) has been increasingly diagnosed. This syndrome is known as a disease that is inherited via an autosomal dominant trait, and the SCN5A mutation has been found in 20-25% of BS patients. Because BS primarily manifests in adulthood, little information is available on BS during childhood. Although there have been several reports on adult BS in Korea, pediatric BS has not been reported. Herein, we report on childhood BS in two families. One infantile BS patient and his family had a novel SCN5A mutation (c.4035G>T, p.W1345C, heterozygote) in domain III of the sodium channel.
Keyword
MeSH Terms
Figure
-
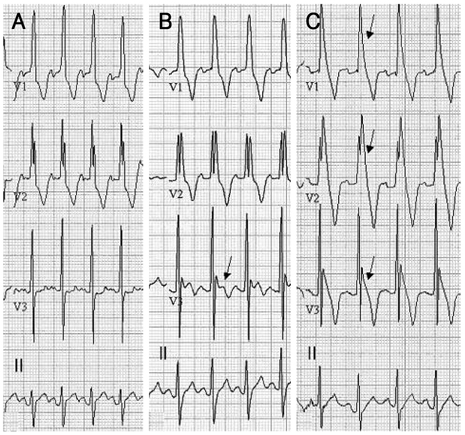
Fig. 1 Serial change of ECG with age in case 1. A: ECG obtained at 1 month of age. Normal sinus rhythm with right axis deviation and possible RBBB pattern are observed. B: ECG at 4 months of age. Significant QRS widening in right precordial leads with saddle back ST elevation in the V3 lead is observed (arrow). C: ECG at 6 months. Definitive ST elevation with T wave inversion of Brugada type 1 pattern is observed (arrows). ECG: electrocardiogram, RBBB: right bundle branch block.
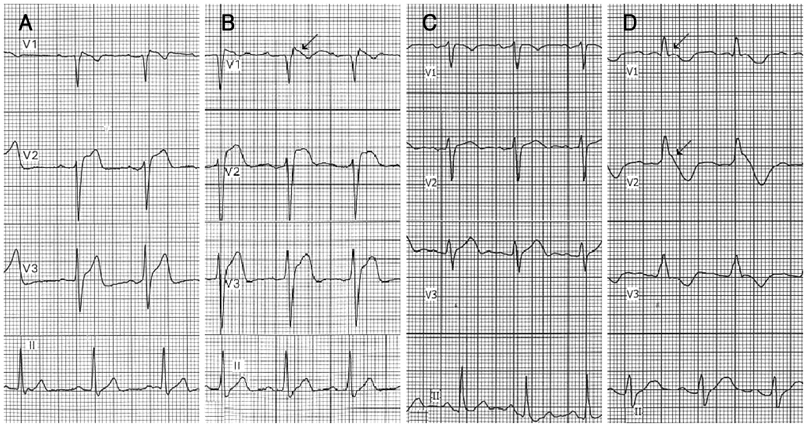
Fig. 2 Parental ECG changes in case 1 on flecainide challenge tests. A: baseline ECG record of the father in case 1. No definite abnormality, but suspicious ST elevation is observed. B: ECG of the father in case 1 obtained after flecainide challenge. Equivocal coved ST-segment elevation followed by T wave inversion (type 1 Brugada pattern) is observed (arrow). C: baseline ECG record of the mother in case 1. Normal sinus rhythm without ST-segment elevation is observed. D: ECG of the mother in case 1 obtained after flecainide challenge. Considerable QRS widening with coved ST-segment elevation followed by T wave inversion (type 1 Brugada pattern) is observed in V1 and V2 leads (arrows). ECG: electrocardiogram.

Fig. 3 DNA sequencing analysis for the cardiac sodium channel (SCN5A). A: study of normal control individual. B: genetic study of case 1 revealed a novel mutation comprised of a G to T base substitution at nucleotide position 4035 that led to replacement of tryptophan by cysteine at codon 1345. C: DNA sequencing analysis of the mother in case 1. The same SCN1A gene mutation as in case 1 was found in the genetic study of the mother. DNA: deoxyribonucleic acid.

Fig. 4 ECG changes of patients in case 2 after the flecainide challenge test. A: ECG of a 12 year old boy after the flecainide challenge test. Typical coved ST-segment elevation followed by T wave inversion is observed on V1 and V2 leads. B: ECG of a 10 year old girl after the flecainide challenge test. Note the typical Brugada pattern ST-segment elevation on V1 and V2 leads. ECG: electrocardiogram.
Cited by 1 articles
-
Prognosis after Implantation of Cardioverter-Defibrillators in Korean Patients with Brugada Syndrome
Myoung Kyun Son, Kyeongmin Byeon, Seung-Jung Park, June Soo Kim, Gi-Byoung Nam, Kee-Joon Choi, You-Ho Kim, Sang Weon Park, Young-Hoon Kim, Hyung Wook Park, Jeong Gwan Cho, Young Keun On
Yonsei Med J. 2014;55(1):37-45. doi: 10.3349/ymj.2014.55.1.37.
Reference
-
1. Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome: a multicenter report. J Am Coll Cardiol. 1992. 20:1391–1396.2. Benito B, Brugada R, Brugada J, Brugada P. Brugada syndrome. Prog Cardiovasc Dis. 2008. 51:1–22.3. Alings M, Wilde A. "Brugada" syndrome: clinical data and suggested pathophysiological mechanism. Circulation. Circulation. 1999. 99:666–673.4. Mattu A, Rogers RL, Kim H, Perron AD, Brady WJ. The Brugada syndrome. Am J Emerg Med. 2003. 21:146–151.5. Kucharczyk-Foltyn A, Sniezek-Maciejewska M, Dymek M, Sadowski J, Janion M. Brugada syndrome: from diagnosis to treatment. Cardiol J. 2007. 14:429–435.6. Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation. 2005. 111:659–670.7. Mivelaz Y, Di Bernardo S, Pruvot E, Meijboom EJ, Sekarski N. Brugada syndrome in childhood: a potential fatal arrhythmia not always recognised by paediatricians: a case report and review of the literature. Eur J Pediatr. 2006. 165:507–511.8. Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999. 100:1660–1666.9. Antzelevitch C. Brugada syndrome. Pacing Clin Electrophysiol. 2006. 29:1130–1159.10. Wilde AA, Antzelevitch C, Borggrefe M, et al. Proposed diagnostic criteria for the Brugada syndrome. Eur Heart J. 2002. 23:1648–1654.11. Chen Q, Kirsch GE, Zhang D, et al. Genetic basis and molecular mechanism for idiopathic ventricular fibrillation. Nature. 1998. 392:293–296.12. Shin CH, Kim NH, Kim HK, et al. A family with a missense mutation in the SCN5A gene. Korean Circ J. 2003. 33:150–154.13. Weiss R, Barmada MM, Nguyen T, et al. Clinical and molecular heterogeneity in the Brugada syndrome: a novel gene locus on chromosome 3. Circulation. 2002. 105:707–713.14. Park SS, Nam GB, Choi KJ, et al. Two cases of sudden cardiac death syndrome associated with right bundle branch block and ST segment elevation. Korean Circ J. 2000. 30:611–616.15. Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol. 2006. 48:e247–e346.16. Probst V, Denjoy I, Meregalli PG, et al. Clinical aspects and prognosis of Brugada syndrome in children. Circulation. 2007. 115:2042–2048.17. Priori SG, Napolitano C, Giordano U, Collisani G, Memmi M. Brugada syndrome and sudden cardiac death in children. Lancet. 2000. 355:808–809.18. Oe H, Takagi M, Tanaka A, et al. Prevalence and clinical course of the juveniles with Brugada-type ECG in Japanese population. Pacing Clin Electrophysiol. 2005. 28:549–554.19. Yamakawa Y, Ishikawa T, Uchino K, et al. Prevalence of right bundle-branch block and right precordial ST-segment elevation (Brugada-type electrocardiogram) in Japanese children. Circ J. 2004. 68:275–279.20. Yoshinaga M, Anan R, Nomura Y, et al. Prevalence and time of appearance of Brugada electrocardiographic pattern in young male adolescents from a three-year follow-up study. Am J Cardiol. 2004. 94:1186–1189.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Idiopathic Brugada ECG Pattern Developed in Relation To Fever
- Anesthesia in a Patient with Brugada Syndrome without a Characteristic ECG Pattern: A case report
- COVID-19 Vaccination-Induced Ventricular Fibrillation in an Afebrile Patient With Brugada Syndrome
- Brugada Syndrome Presenting With Convulsion in the Emergency Department: A Case Report
- Brugada Syndrome
