Primary Lymphedema of the Lower Limb: The Clinical Utility of Single Photon Emission Computed Tomography/CT
- Affiliations
-
- 1Department of Nuclear Medicine, Ludwig-Maximilians-University of Munich, Muenchen D-81377, Germany. mayo.weiss@med.uni-muenchen.de
- 2Department of Micro-, Hand-, and Reconstructive Surgery, Ludwig-Maximilians-University of Munich, Muenchen D-81377, Germany.
- KMID: 2069999
- DOI: http://doi.org/10.3348/kjr.2015.16.1.188
Abstract
OBJECTIVE
The aim of this prospective study was to determine whether the additional use of the single photon emission computed tomography/CT (SPECT/CT) technique improves the diagnostic value of planar lymphoscintigraphy in patients presenting with primary lymph edema of the lower limb.
MATERIALS AND METHODS
For a defined period of three years (April 2011-April 2014) a total of 34 consecutive patients (28 females; age range, 27-83 years) presenting with swelling of the leg(s) suspicious of (uni- or bilateral, proximal or distal) primary lymphedema were prospectively examined by planar lymphoscintigraphy (lower limbs, n = 67) and the tomographic SPECT/CT technique (anatomical sides, n = 65).
RESULTS
In comparison to pathological planar scintigraphic findings, the addition of SPECT/CT provided relevant additional information regarding the presence of dermal backflow (86%), the anatomical extent of lymphatic disorders (64%), the presence or absence of lymph nodes (46%), and the visualization of lymph vessels (4%).
CONCLUSION
As an adjunct to planar lymphoscintigraphy, SPECT/CT specifies the anatomical correlation of lymphatic disorders and thus improves assessment of the extent of pathology due to the particular advantages of tomographic separation of overlapping sources. The interpretation of scintigraphic data benefits not only in baseline diagnosis, but also in physiotherapeutical and microsurgical treatments of primary lymphedema.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Female
Humans
Lower Extremity/anatomy & histology/*radiography
Lymphatic Vessels/radiography
Lymphedema/*diagnosis/radiography
Lymphoscintigraphy
Middle Aged
Radiopharmaceuticals/diagnostic use
Retrospective Studies
Tomography, Emission-Computed, Single-Photon
Tomography, X-Ray Computed
Radiopharmaceuticals
Figure
-
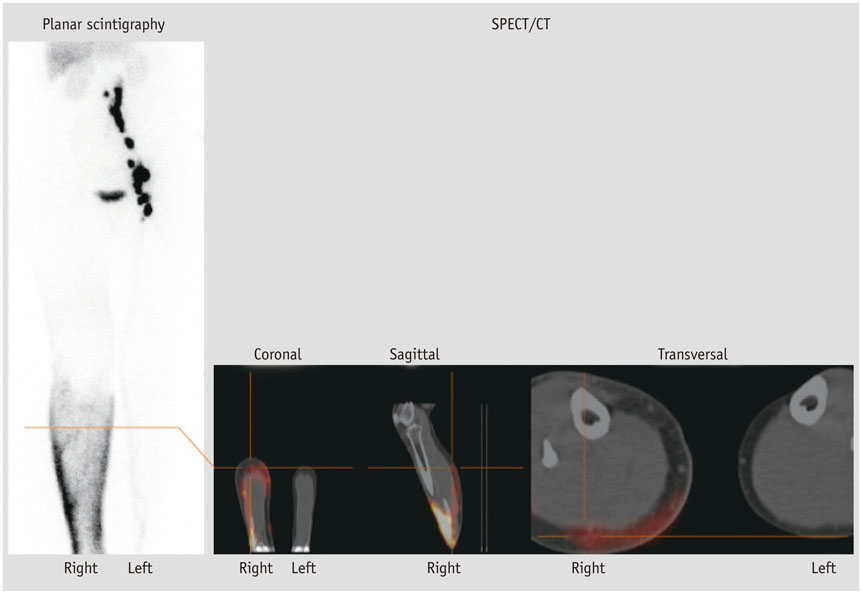
Fig. 1 60-year-old female patient with clinically swelling of lower right leg suspicious for primary lymphedema. Lymphatic transport disorders (diffuse distribution of radiopharmaceutical at right lower leg, delayed/missing inguinal lymph nodes of right leg, transport-index 39) were properly detected in planar lymphoscintigraphy (4.5 hours after injection), but only tomographic acquisition by means of single photon emission computed tomography/CT (SPECT/CT) confirmed "dermal backflow" at posterior right lower leg (red colored); additional value of SPECT/CT in terms of dermal backflow consists of three-dimensional spatial resolution and definable location of anatomical margins. Physiological lymph transport and distinct visualization of inguinal and iliacal lymph nodes of left leg.
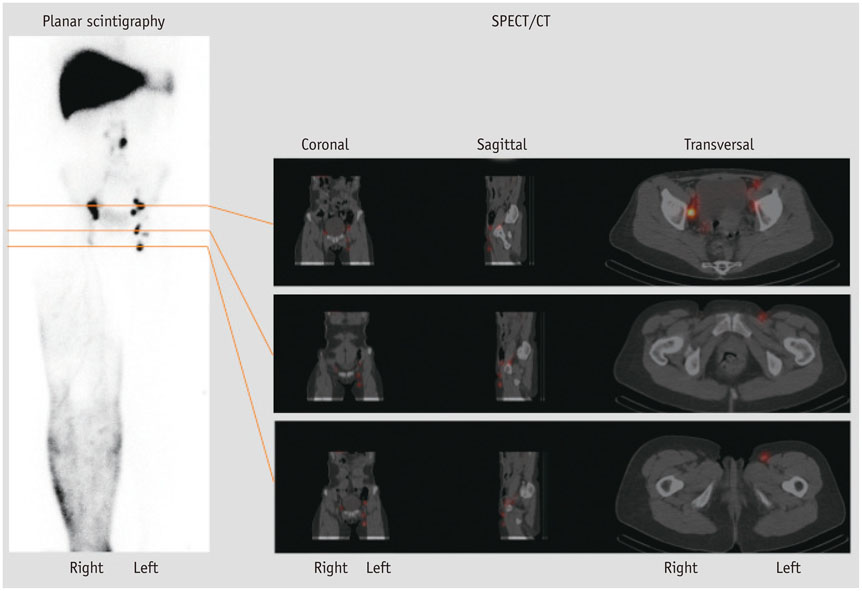
Fig. 2 46-year-old female patient with clinically swelling of right leg suspicious for primary lymphedema. Planar lymphoscintigraphy clearly depicted diffuse distribution of radiopharmaceutical at right lower leg and upper leg. In comparison to contralateral side, likely decreased number of inguinal lymph nodes could be suspected, which was reliably confirmed with three-dimensional anatomical correlation by means of single photon emission computed tomography/CT (SPECT/CT). While planar scintigraphy is limited to functionally demonstrate (inguinal) lymph nodes, CT-component of SPECT/CT serves to verify morphological presence of lymph nodes in this area. Physiological lymph transport and distinct visualization of inguinal lymph nodes of left leg.

Fig. 3 65-year-old female patient with clinically swelling of lower left leg suspicious for primary lymphedema. Lymphatic transport disorders (e.g., diffuse distribution of radiopharmaceutical at left lower leg, delayed/missing inguinal lymph nodes of left leg, transport-index 11) were properly detected in planar lymphoscintigraphy (4 hours after injection); due to its three-dimensional imaging options, additionally performed single photon emission computed tomography/CT (SPECT/CT) enables differentiation of anterior versus posterior lymph transport, thus providing accurate anatomic correlation and functional assessment of extent of edema (red colored). Planar lymphoscintigraphy cannot provide these special kinds of morphological information. Physiological lymph transport and distinct visualization of inguinal and iliacal lymph nodes of right leg.
Reference
-
1. Pecking AP, Albérini JL, Wartski M, Edeline V, Cluzan RV. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008; 41:1–10.2. Weiss M, Gildehaus FJ, Brinkbäumer K, Makowski M, Hahn K. [Lymph kinetics with technetium-99m labeled radiopharmaceuticals. Animal studies]. Nuklearmedizin. 2005; 44:156–116.3. Weiss M, Baumeister RG, Hahn K. Dynamic lymph flow imaging in patients with oedema of the lower limb for evaluation of the functional outcome after autologous lymph vessel transplantation: an 8-year follow-up study. Eur J Nucl Med Mol Imaging. 2003; 30:202–206.4. Baulieu F, Bourgeois P, Maruani A, Belgrado JP, Tauveron V, Lorette G, et al. Contributions of SPECT/CT imaging to the lymphoscintigraphic investigations of the lower limb lymphedema. Lymphology. 2013; 46:106–119.5. International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2013 Consensus Document of the International Society of Lymphology. Lymphology. 2013; 46:1–11.6. Kleinhans E, Baumeister RG, Hahn D, Siuda S, Büll U, Moser E. Evaluation of transport kinetics in lymphoscintigraphy: follow-up study in patients with transplanted lymphatic vessels. Eur J Nucl Med. 1985; 10:349–352.7. Weiss M, Baumeister RG, Tatsch K, Hahn K. [Lymphoscintigraphy for non-invasive long term follow-up of functional outcome in patients with autologous lymph vessel transplantation]. Nuklearmedizin. 1996; 35:236–242.8. Bourgeois P. Scintigraphic investigations of the lymphatic system: the influence of injected volume and quantity of labeled colloidal tracer. J Nucl Med. 2007; 48:693–695.9. Monnin-Delhom ED, Gallix BP, Achard C, Bruel JM, Janbon C. High resolution unenhanced computed tomography in patients with swollen legs. Lymphology. 2002; 35:121–128.10. Baumeister RG, Seifert J, Hahn D. Autotransplantation of lymphatic vessels. Lancet. 1981; 1:147.11. O'Mahony S, Rose SL, Chilvers AJ, Ballinger JR, Solanki CK, Barber RW, et al. Finding an optimal method for imaging lymphatic vessels of the upper limb. Eur J Nucl Med Mol Imaging. 2004; 31:555–563.12. Bocher M, Balan A, Krausz Y, Shrem Y, Lonn A, Wilk M, et al. Gamma camera-mounted anatomical X-ray tomography: technology, system characteristics and first images. Eur J Nucl Med. 2000; 27:619–627.13. Wallmichrath J, Baumeister R, Giunta RE, Notohamiprodjo M, Frick A. [Update on special surgical approaches in the therapy for lymphedemas]. Handchir Mikrochir Plast Chir. 2012; 44:334–342.14. Weiss M, Landrock S, Wallmichrath J, Baumeister RG, Bartenstein P, Frick A. [The clinical yield of SPECT/CT for the assessment of lymphatic transport disorders. First experiences]. Nuklearmedizin. 2013; 52:235–224.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nuclear Medicine Imaging in Rheumatic Diseases
- A Case of Orbital Cavernous Hemangioma with Multiple Intra c ranial Lesions
- RE: Novel Application of Quantitative Single-Photon Emission Computed Tomography/Computed Tomography to Predict Early Response to Methimazole in Graves' Disease
- Extramedullary Pulmonary Hematopoiesis Causing Pulmonary Hypertension and Severe Tricuspid Regurgitation Detected by Technetium-99m Sulfur Colloid Bone Marrow Scan and Single-Photon Emission Computed Tomography/CT
- Clinical Applications of Technetium-99m Quantitative Single-Photon Emission Computed Tomography/Computed Tomography
