MR Imaging Appearances of Soft Tissue Flaps Following Reconstructive Surgery of the Lower Extremity
- Affiliations
-
- 1Department of Radiology, Hospital Baden, Baden 5405, Switzerland. dr.o.magerkurth@gmail.com
- 2Department of Radiology, University of Michigan Hospitals, Ann Arbor, MI 48109, USA.
- KMID: 2069995
- DOI: http://doi.org/10.3348/kjr.2015.16.1.160
Abstract
- MR imaging appearances of different types of reconstructive muscle flaps following reconstructive surgery of the lower extremity with associated post-surgical changes due to altered anatomy, radiation, and potential complications, can be challenging. A multidisciplinary therapeutic approach to tumors allows for limb salvage therapy in a majority of the patients. Decision-making for specific types of soft tissue reconstruction is based on the body region affected, as well as the size and complexity of the defect. Hematomas and infections are early complications that can jeopardize flap viability. The local recurrence of a tumor within six months after a complete resection with confirmed tumor-free margins and adjuvant radiation therapy is rare. Identification of a new lesion similar to the initial tumor favors a finding of tumor recurrence.
MeSH Terms
-
Adult
Female
Hematoma/etiology
Humans
Limb Salvage
Lower Extremity/anatomy & histology/radiography/*surgery
*Magnetic Resonance Imaging
Male
Middle Aged
Neoplasm Recurrence, Local
Reconstructive Surgical Procedures
Sarcoma/radiotherapy/*surgery
Soft Tissue Infections/radiography/*surgery
Soft Tissue Injuries/radiography/*surgery
Soft Tissue Neoplasms/radiotherapy/*surgery
Surgical Flaps/adverse effects
Figure
-

Fig. 1 63-year-old woman with right groin high-grade fibromyxoid sarcoma with extensive central necrosis and tensor fascia lata myocutaneous flap following tumor resection. A. Preoperative axial gadolinium-enhanced T1-weighted MR image with fat saturation depicts tumor (T). Largely non-enhancing myxoid tumor infiltrates skin and underlying sartorius muscle (*) with loss of fat plane at tumor-muscle interface. B. Axial proton density-weighted MR image 6 months after surgery and radiation. Note postsurgical anteromedial shift of tensor fascia lata muscle (M) and coverage of soft tissue defect by tensor fascia lata myocutaneous flap (arrows). Fem = femur

Fig. 2 57-year-old paraplegic female with right ischial osteomyelitis and pressure ulcer, underwent partial ischiectomy and wound closure with gluteus maximus muscle flap. A. Preoperative axial gadolinium enhanced T1-weighted image with fat saturation. Note periostal reaction and loss of cortical outline of right ischium (*). Also, note extensive right gluteal hyper intensity interpreted as edema and abscess (arrow) posterolateral to right ischium (*). B. Postoperative coronal T1-weighted image. Persistent changes of osteomyelitis (*) show low signal in right ischium. C. Postoperative axial T2-weighted image with fat saturation. Note inferomedial relocation of gluteus maximus muscle (M) on right, resulting in significant soft tissue asymmetry (involving both muscle and fat) compared to normal left ischial region. D. Postoperative axial T1-weighted image at same level showing resolving ischial bone changes (*) following additional antibiotic therapy. S = symphysis pubis

Fig. 3 39-year-old man with proximal inner thigh fibromyxoid sarcoma and wound closure with myocutaneous gracilis flap following tumor resection. A. Axial proton density-weighted MR image after incomplete resection showing scar (arrow) on inner thigh. Markers (*) were placed on skin surface adjacent to scar. B. Axial T1-weighted MR image following complete re-resection shows relocation and stretching of gracilis muscle (M) and subcutaneous fat (arrows) which have been shifted to cover surgical defect. Fem = right femur
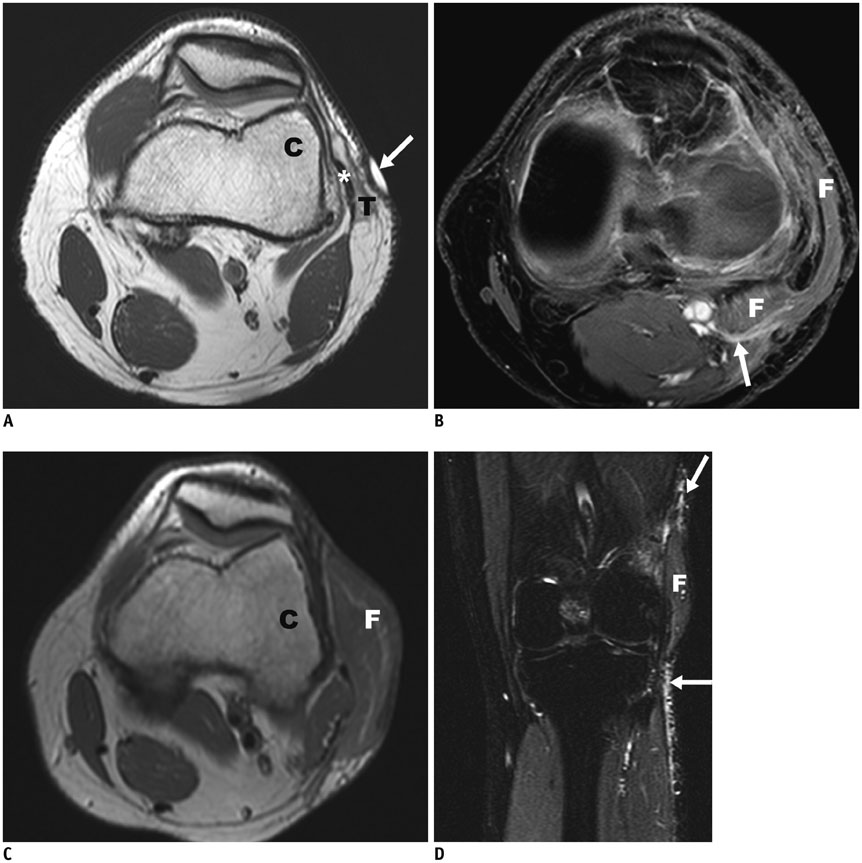
Fig. 4 30-year-old woman with excision of high-grade myxofibrosarcoma and wound closure with lateral gastrocnemius flap. A. Axial proton density-weighted MR image shows tumor (T) with infiltration of skin and iliotibial band of knee (*). Cutaneous marker (arrow). B. Axial gadolinium enhanced T1-weighted MR image with fat saturation shows vascular pedicle (arrow) of gastrocnemius flap (F). C. Axial proton density-weighted MR image more proximally at level of lateral femoral condyle (C) shows the flap (F) covering lateral post-excisional defect. D. Coronal short tau inversion recovery image shows craniocaudal extension of flap (F). Note edema of skin (arrows) following radiation therapy.

Fig. 5 25-year-old man with crush injury of lower leg, comminuted calcaneus fracture, and compartment syndrome. After fasciotomy, delayed closure of defect with free gracilis flap was performed. A. Coronal T1-weighted MR image shows extent (arrows) of gracilis muscle flap (F) in medial and plantar aspects of midfoot. B. Sagittal T2-weighted MR image with fat saturation shows longitudinal extent of flap (F) overlying the proximal plantar foot. C = 2nd cuneiform bone

Fig. 6 57-year-old woman with severe crush injury, comminuted fractures of tibia, fibula, and large open wound with exposed tibia extending from upper tibia to ankle. Wound closure was performed with rectus abdominis free flap. A. Anteroposterior radiograph of lower leg shows multiple fractures of tibia and fibula. Note extensive soft tissue abnormality with anteromedial defect (arrows) and emphysema (*). B. Axial CT scan proximal to fibular fracture. Note soft tissue emphysema (*) anterolaterally and overlying skin defect (arrow). C. Anteroposterior radiograph after soft tissue reconstruction shows prominent lobulated soft tissue medial to distal tibia, which represents soft tissue flap (F). Also note internal fixation of tibial fracture (*) with improved alignment. G = gauze, T = left tibia

Fig. 7 57-year-old woman with excision of distal lower leg high-grade myxofibrosarcoma and wound closure with latissimus dorsi free flap. A. Axial T1-weighted MR image after tumor excision. Note large skin defect (arrows) adjacent to fibula (*) with peroneus muscle exposed. B. Axial T1-weighted MR image 1 year after reconstruction with optimal coverage of fibula. Note extensive, but expected, fatty infiltration of muscle flap (F). T = left tibia

Fig. 8 48-year-old woman after resection of high-grade myxofibrosarcoma and wound closure with lateral gastrocnemius flap. Coronal T2-weighted MR image (A) and axial T2-weighted MR image (B) with fat saturation. Note fluid collection (*) proximal to flap (F), located at undersurface of graft, extending proximally. arrow = cutaneous marker. C = left lateral femoral condyle, Fem = left femur

Fig. 9 47-year-old male patient with lower leg high-grade undifferentiated pleomorphic sarcoma and subsequent postsurgical defect covered with combined myocutaneous soleus/medial gastrocnemius flap. A. Preoperative axial gadolinium enhanced T1-weighted MR image with fat saturation shows enhancing tumor (T) abutting tibia and underlying soleus muscle (M). * = right fibula. B. Post-operative axial gadolinium enhanced T1-weighted MR image with fat saturation shows patchy enhancement of flap (F) and adjacent soft tissue, without mass effect. Even though non-specific, this was clinically interpreted as infection in keeping with clinical presentation and findings.

Fig. 10 55-year-old man with myxoid liposarcoma and post-surgical wound covered with lateral gastrocnemius flap after resection. Axial T2-weighted MR image with fat saturation shows homogenous hyperintensity (arrows) of irradiated region with well-defined margins best noted anteriorly. This differs from patchy enhancement (Fig. 9) attributed to infection. There is also some joint effusion in lateral recess of knee joint. Fem = left femur

Fig. 11 59-year-old woman with recurrence of high grade myxofibroma after initial wound closure by medial gastrocnemius flap and re-excision closure with free latissimus dorsi flap. A. Coronal T1-weighted MR image shows lobular and heterogeneous appearance of recurrent tumor (T), which extends proximally and medially to gastrocnemius flap (F). B. Coronal T1-weighted MR image after re-excision and coverage of defect with free latissimus dorsi flap (F), which extends from medial thigh. C. Corresponding axial T1-weighted MR image after re-excision and coverage of popliteal region with free latissimus dorsi flap (F). C = medial femoral condyle, Tib = left tibia
Reference
-
1. Bannasch H, Haivas I, Momeni A, Stark GB. Oncosurgical and reconstructive concepts in the treatment of soft tissue sarcomas: a retrospective analysis. Arch Orthop Trauma Surg. 2009; 129:43–49.2. Drake DB. Reconstruction for limb-sparing procedures in soft-tissue sarcomas of the extremities. Clin Plast Surg. 1995; 22:123–128.3. Heller L, Kronowitz SJ. Lower extremity reconstruction. J Surg Oncol. 2006; 94:479–489.4. Misra A, Mistry N, Grimer R, Peart F. The management of soft tissue sarcoma. J Plast Reconstr Aesthet Surg. 2009; 62:161–174.5. Morii T, Mochizuki K, Takushima A, Okazaki M, Satomi K. Soft tissue reconstruction using vascularized tissue transplantation following resection of musculoskeletal sarcoma: evaluation of oncologic and functional outcomes in 55 cases. Ann Plast Surg. 2009; 62:252–257.6. Serletti JM, Carras AJ, O'Keefe RJ, Rosier RN. Functional outcome after soft-tissue reconstruction for limb salvage after sarcoma surgery. Plast Reconstr Surg. 1998; 102:1576–1583. discussion 1584-1585.7. Karakousis CP, Proimakis C, Walsh DL. Primary soft tissue sarcoma of the extremities in adults. Br J Surg. 1995; 82:1208–1212.8. Popov P, Tukiainen E, Asko-Seljavaara S, Huuhtanen R, Virolainen M, Virkkunen P, et al. Soft-tissue sarcomas of the upper extremity: surgical treatment and outcome. Plast Reconstr Surg. 2004; 113:222–230. discussion 231-232.9. Zenn MR, Levin LS. Microvascular reconstruction of the lower extremity. Semin Surg Oncol. 2000; 19:272–281.10. Parrett BM, Talbot SG, Pribaz JJ, Lee BT. A review of local and regional flaps for distal leg reconstruction. J Reconstr Microsurg. 2009; 25:445–455.11. Heller L, Levin LS. Lower extremity microsurgical reconstruction. Plast Reconstr Surg. 2001; 108:1029–1041. quiz 1042.12. Moreira-Gonzalez A, Djohan R, Lohman R. Considerations surrounding reconstruction after resection of musculoskeletal sarcomas. Cleve Clin J Med. 2010; 77:Suppl 1. S18–S22.13. Achauer B, Eriksson E, Guyuron B, Coleman IJ, Russel R, Vander Kolk C. Plastic surgery: indications, operations, and outcomes. Saint-Louis: Mosby;2000. p. 475–496.14. Parrett BM, Pribaz JJ, Matros E, Przylecki W, Sampson CE, Orgill DP. Risk analysis for the reverse sural fasciocutaneous flap in distal leg reconstruction. Plast Reconstr Surg. 2009; 123:1499–1504.15. Peat BG, Bell RS, Davis A, O'Sullivan B, Mahoney J, Manktelow RT, et al. Wound-healing complications after soft-tissue sarcoma surgery. Plast Reconstr Surg. 1994; 93:980–987.16. Trecek J, Sundaram M. Radiologic case study. Extensive hematoma of the vastus intermedius showing components of subacute and chronic hemorrhage with associated myositis of the vastus intermedius and medialis. Orthopedics. 2007; 30:806880–881.17. Varma DG, Jackson EF, Pollock RE, Benjamin RS. Soft-tissue sarcoma of the extremities. MR appearance of post-treatment changes and local recurrences. Magn Reson Imaging Clin N Am. 1995; 3:695–712.18. Poon-Chue A, Menendez L, Gerstner MM, Colletti P, Terk M. MRI evaluation of post-operative seromas in extremity soft tissue sarcomas. Skeletal Radiol. 1999; 28:279–282.19. Ferguson PC. Surgical considerations for management of distal extremity soft tissue sarcomas. Curr Opin Oncol. 2005; 17:366–369.20. Vanel D, Lacombe MJ, Couanet D, Kalifa C, Spielmann M, Genin J. Musculoskeletal tumors: follow-up with MR imaging after treatment with surgery and radiation therapy. Radiology. 1987; 164:243–245.21. Costelloe CM, Kumar R, Yasko AW, Murphy WA Jr, Stafford RJ, Lewis VO, et al. Imaging characteristics of locally recurrent tumors of bone. AJR Am J Roentgenol. 2007; 188:855–863.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reconstruction of soft tissue defect in the lower extremity with free flaps
- A Combined Scapular Flap and Latissimus Dorsi Flap
- Reconstruction of soft tissue injury of lower extremity with free flap transfer
- Reconstruction of lower extremity by fibular free flaps
- Reconstruction of Lower Extremities using Anterolateral thigh Perforator Free Flaps
