Effect of Papillary Muscles and Trabeculae on Left Ventricular Measurement Using Cardiovascular Magnetic Resonance Imaging in Patients with Hypertrophic Cardiomyopathy
- Affiliations
-
- 1Department of Radiology, Cardiovascular Division, Seoul National University Hospital, Seoul 110-744, Korea. whal.lee@gmail.com
- 2Department of Internal Medicine, Cardiovascular Division, Seoul National University Hospital, Seoul 110-744, Korea.
- KMID: 2069980
- DOI: http://doi.org/10.3348/kjr.2015.16.1.4
Abstract
OBJECTIVE
To evaluate the influence of papillary muscles and trabeculae on left ventricular (LV) cardiovascular magnetic resonance (CMR) analysis using three methods of cavity delineation (classic or modified inclusion methods, and the exclusion method) in patients with hypertrophic cardiomyopathy (HCM).
MATERIALS AND METHODS
This retrospective study included 20 consecutive HCM patients who underwent 1.5-T CMR imaging with short-axis cine stacks of the entire LV. LV measurements were performed using three different methods of manual cavity delineation of the endocardial and epicardial contours: method A, presumed endocardial boundary as seen on short-axis cine images; method B, including solely the cavity and closely adjacent trabeculae; or method C, excluding papillary muscles and trabeculae. Ascending aorta forward flow was measured as reference for LV-stroke volume (SV). Interobserver reproducibility was assessed using intraclass correlation coefficients.
RESULTS
Method A showed larger end-diastole and end-systole volumes (largest percentage differences of 25% and 68%, respectively, p < 0.05), compared with method C. The ejection fraction was 55.7 +/- 6.9% for method A, 68.6 +/- 8.4% for B, and 71.7 +/- 7.0% for C (p < 0.001). Mean mass was also significantly different: 164.6 +/- 47.4 g for A, 176.5 +/- 50.5 g for B, and 199.6 +/- 53.2 g for C (p < 0.001). LV-SV error was largest with method B (p < 0.001). No difference in interobserver agreement was observed (p > 0.05).
CONCLUSION
In HCM patients, LV measurements are strikingly different dependent on whether papillary muscles and trabeculae are included or excluded. Therefore, a consistent method of LV cavity delineation may be crucial during longitudinal follow-up to avoid misinterpretation and erroneous clinical decision-making.
Keyword
MeSH Terms
Figure
-
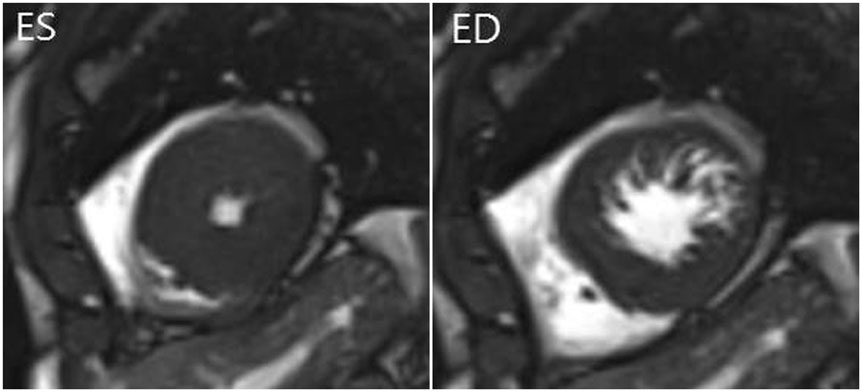
Fig. 1 End-systole (ES) and end-diastole (ED) cine MR images in 54-year-old man with hypertrophic cardiomyopathy. Trabeculae are hypertrophied and abundant, and are difficult to discern from compact myocardium at ES phase.
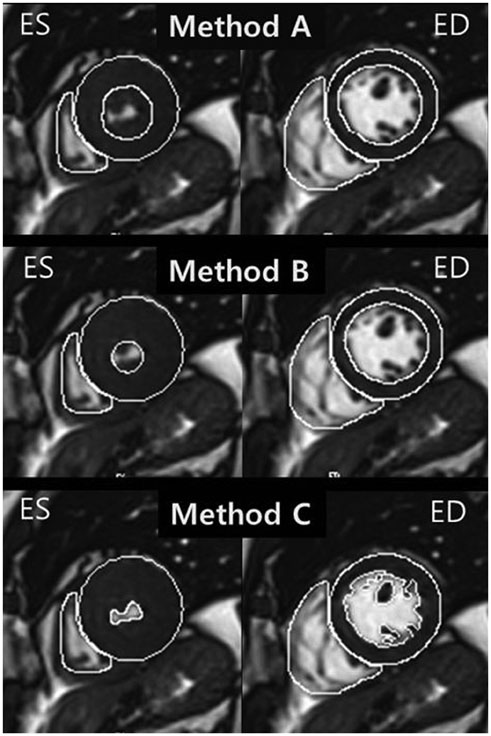
Fig. 2 Representative example of endocardial contouring using three methods in 51-year-old man with hypertrophic cardiomyopathy. Method A indicates classic method for inclusion of trabeculae in left ventricular (LV) cavity volume. Single short-axis-view true FISP MR images at end-diastolic (ED) and end-systolic (ES) phases show inclusion of trabeculae in LV cavity volume. Method B includes closely adjacent trabeculae in LV cavity volume. ES image shows inclusion of trabeculae in LV cavity volume similar to method A. However, endocardial contour is smaller, based solely on cavity and closely adjacent trabeculae. Method C indicates classic method for exclusion of trabeculae from LV cavity volume. Trabeculae were completely excluded from cavity volume.
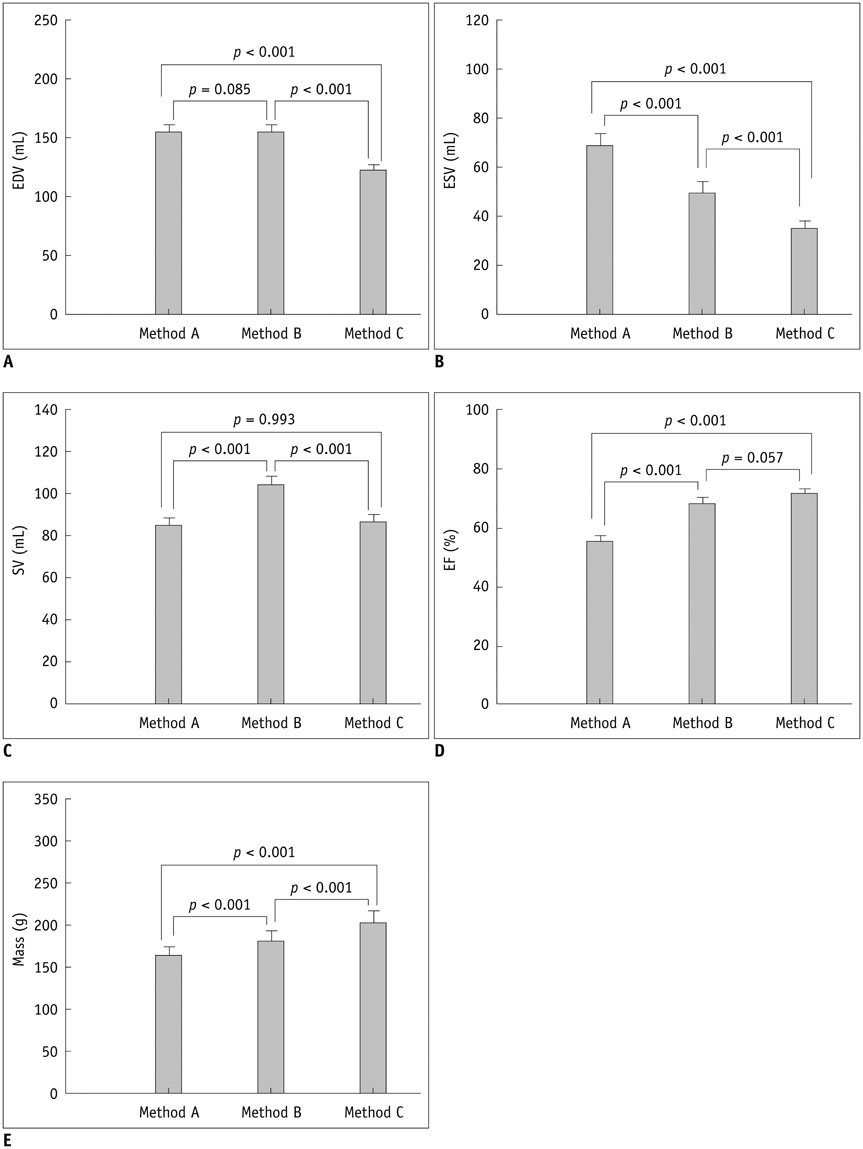
Fig. 3 Bar graphs showing mean values of left ventricular measures using three different methods. Vertical lines indicate standard error. A. End-diastolic volume (EDV). B. End-systolic volume (ESV). C. Stroke volume (SV). D. Ejection fraction (EF). E. Myocardial mass.
Cited by 1 articles
-
Cardiac CT for Measurement of Right Ventricular Volume and Function in Comparison with Cardiac MRI: A Meta-Analysis
Jin Young Kim, Young Joo Suh, Kyunghwa Han, Young Jin Kim, Byoung Wook Choi
Korean J Radiol. 2020;21(4):450-461. doi: 10.3348/kjr.2019.0499.
Reference
-
1. Biederman RW, Magovern JA, Grant SB, Williams RB, Yamrozik JA, Vido DA, et al. LV reverse remodeling imparted by aortic valve replacement for severe aortic stenosis; is it durable? A cardiovascular MRI study sponsored by the American Heart Association. J Cardiothorac Surg. 2011; 6:53.2. Lorenz CH, Walker ES, Graham TP Jr, Powers TA. Right ventricular performance and mass by use of cine MRI late after atrial repair of transposition of the great arteries. Circulation. 1995; 92:9 Suppl. II233–II239.3. Oosterhof T, Tulevski II, Vliegen HW, Spijkerboer AM, Mulder BJ. Effects of volume and/or pressure overload secondary to congenital heart disease (tetralogy of fallot or pulmonary stenosis) on right ventricular function using cardiovascular magnetic resonance and B-type natriuretic peptide levels. Am J Cardiol. 2006; 97:1051–1055.4. Pattynama PM, Lamb HJ, Van der Velde EA, Van der Geest RJ, Van der Wall EE, De Roos A. Reproducibility of MRI-derived measurements of right ventricular volumes and myocardial mass. Magn Reson Imaging. 1995; 13:53–63.5. Lorenz CH, Walker ES, Morgan VL, Klein SS, Graham TP Jr. Normal human right and left ventricular mass, systolic function, and gender differences by cine magnetic resonance imaging. J Cardiovasc Magn Reson. 1999; 1:7–21.6. Rominger MB, Bachmann GF, Pabst W, Rau WS. Right ventricular volumes and ejection fraction with fast cine MR imaging in breath-hold technique: applicability, normal values from 52 volunteers, and evaluation of 325 adult cardiac patients. J Magn Reson Imaging. 1999; 10:908–918.7. Sievers B, Kirchberg S, Bakan A, Franken U, Trappe HJ. Impact of papillary muscles in ventricular volume and ejection fraction assessment by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2004; 6:9–16.8. Papavassiliu T, Kühl HP, Schröder M, Süselbeck T, Bondarenko O, Böhm CK, et al. Effect of endocardial trabeculae on left ventricular measurements and measurement reproducibility at cardiovascular MR imaging. Radiology. 2005; 236:57–64.9. Winter MM, Bernink FJ, Groenink M, Bouma BJ, van Dijk AP, Helbing WA, et al. Evaluating the systemic right ventricle by CMR: the importance of consistent and reproducible delineation of the cavity. J Cardiovasc Magn Reson. 2008; 10:40.10. Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011; 124:e783–e831.11. Goo JM, Tongdee T, Tongdee R, Yeo K, Hildebolt CF, Bae KT. Volumetric measurement of synthetic lung nodules with multi-detector row CT: effect of various image reconstruction parameters and segmentation thresholds on measurement accuracy. Radiology. 2005; 235:850–856.12. Donner A, Zou G. Testing the equality of dependent intraclass correlation coefficients. J R Stati Soc Ser D Stat. 2002; 51:367–379.13. McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. 1996; 1:30–46.14. Didier D, Ratib O, Lerch R, Friedli B. Detection and quantification of valvular heart disease with dynamic cardiac MR imaging. Radiographics. 2000; 20:1279–1299. discussion 1299-1301.15. Lotz J, Meier C, Leppert A, Galanski M. Cardiovascular flow measurement with phase-contrast MR imaging: basic facts and implementation. Radiographics. 2002; 22:651–671.16. Efthimiadis GK, Meditskou S, Giannakoulas G, Parcharidou D, Styliadis I, Mochlas S, et al. Normal systolic function in hypertrophic cardiomyopathy: reality or myth? Eur Heart J. 2008; 29:948. author reply 949.17. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002; 287:1308–1320.18. Olivotto I, Maron MS, Autore C, Lesser JR, Rega L, Casolo G, et al. Assessment and significance of left ventricular mass by cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2008; 52:559–566.19. Reichek N, Gupta D. Hypertrophic cardiomyopathy: cardiac magnetic resonance imaging changes the paradigm. J Am Coll Cardiol. 2008; 52:567–568.20. Beerbaum P, Barth P, Kropf S, Sarikouch S, Kelter-Kloepping A, Franke D, et al. Cardiac function by MRI in congenital heart disease: impact of consensus training on interinstitutional variance. J Magn Reson Imaging. 2009; 30:956–966.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Late Gadolinium Enhancement of the Anterolateral Papillary Muscle in a Patient With Acute Myocardial Infarction, Atrial Fibrillation and Hypertrophic Cardiomyopathy
- A Case of Regressed Apical Hypertrophic Cardiomyopathy
- Sigmoid Septum and Aberrant Calcified Papillary Muscle in the Setting of Advanced Hypertrophic Cardiomyopathy: An Unusual Life-threatening Coalescence
- Mid-Ventricular Obstructive Hypertrophic Cardiomyopathy Associated with an Apical Aneurysm: Evaluation of Possible Causes of Aneurysm Formation
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
