J Cardiovasc Ultrasound.
2015 Sep;23(3):136-142. 10.4250/jcu.2015.23.3.136.
Clinical and Echocardiographic Factors Affecting Tricuspid Regurgitation Severity in the Patients with Lone Atrial Fibrillation
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Inha University Hospital, Incheon, Korea. sshin@inha.ac.kr
- KMID: 2068723
- DOI: http://doi.org/10.4250/jcu.2015.23.3.136
Abstract
- BACKGROUND
Atrial fibrillation (AF) can be a risk factor for development of significant tricuspid regurgitation (TR). We investigated which clinical and echocardiographic parameters were related to severity of functional TR in patients with lone AF.
METHODS
A total of 89 patients with lone AF were enrolled (75 +/- 11 years; 48% male): 13 patients with severe TR, 36 patients with moderate TR, and 40 consecutive patients with less than mild TR. Clinical parameters and echocardiographic measurements including right ventricular (RV) remodeling and function were evaluated.
RESULTS
Patients with more severe TR were older and had more frequently persistent AF (each p < 0.001). TR severity was related to right atrial area and tricuspid annular systolic diameter (all p < 0.001). The patients with moderate or severe TR had larger left atrial (LA) volume and increased systolic pulmonary artery pressure (SPAP) than the patients with mild TR (p = 0.04 for LA volume; p < 0.001 for SPAP). RV remodeling represented by enlarged RV area and increased tenting height was more prominent in severe TR than mild or moderate TR (all p < 0.001). Multivariate analysis showed type of AF, LA volume, tricuspid annular diameter and tenting height remained as a significant determinants of severe TR. In addition, tenting height was independently associated with the presence of severe TR (p = 0.04).
CONCLUSION
In patients with lone AF, TR was related to type of AF, LA volume, tricuspid annular diameter and RV remodeling. Especially, tricuspid valvular tethering seemed to be independently associated with development of severe functional TR.
MeSH Terms
Figure
-
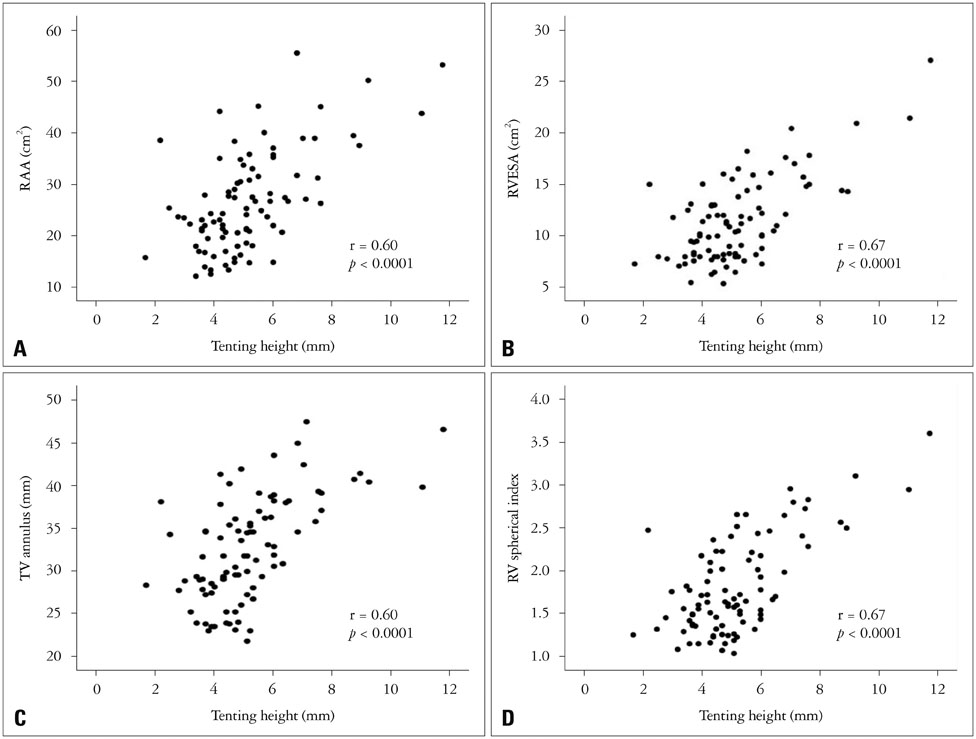
Fig. 1 Relationship between tenting height and RAA (A), RVESA (B), TV annulus (C), and RV spherical index (D). RAA: right atrial area, RV: right ventricle, RVESA: right ventricular end-systolic area, TV: tricuspid valve.
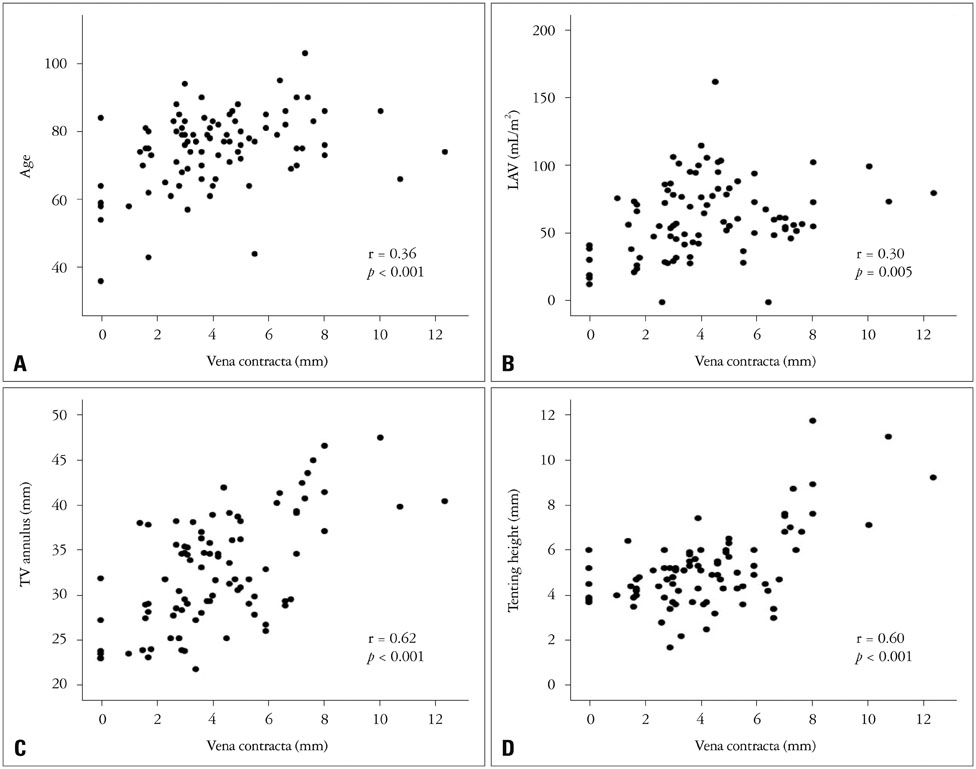
Fig. 2 Relationship between vena contracta and age (A), LAV (B), TV annulus (C), and tenting height (D). LAV: left atrial volume, TV: tricuspid valve
Cited by 2 articles
-
Tricuspid Regurgitation, Isn't It Time to Look Around the Valve Rather Than the Valve Itself?
Seung-Pyo Lee
J Cardiovasc Ultrasound. 2015;23(3):134-135. doi: 10.4250/jcu.2015.23.3.134.Current Unmet Needs and Clues to the Solution in the Management of Tricuspid Regurgitation
Byung Joo Sun, Jae-Hyeong Park
Korean Circ J. 2022;52(6):414-428. doi: 10.4070/kcj.2022.0117.
Reference
-
1. Badano LP, Muraru D, Enriquez-Sarano M. Assessment of functional tricuspid regurgitation. Eur Heart J. 2013; 34:1875–1885.
Article2. Nath J, Foster E, Heidenreich PA. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405–409.
Article3. Topilsky Y, Khanna A, Le Tourneau T, Park S, Michelena H, Suri R, Mahoney DW, Enriquez-Sarano M. Clinical context and mechanism of functional tricuspid regurgitation in patients with and without pulmonary hypertension. Circ Cardiovasc Imaging. 2012; 5:314–323.
Article4. Mutlak D, Lessick J, Reisner SA, Aronson D, Dabbah S, Agmon Y. Echocardiography-based spectrum of severe tricuspid regurgitation: the frequency of apparently idiopathic tricuspid regurgitation. J Am Soc Echocardiogr. 2007; 20:405–408.
Article5. Sagie A, Schwammenthal E, Padial LR, Vazquez de Prada JA, Weyman AE, Levine RA. Determinants of functional tricuspid regurgitation in incomplete tricuspid valve closure: Doppler color flow study of 109 patients. J Am Coll Cardiol. 1994; 24:446–453.
Article6. Kim HK, Lee SP, Kim YJ, Sohn DW. Tricuspid regurgitation: clinical importance and its optimal surgical timing. J Cardiovasc Ultrasound. 2013; 21:1–9.
Article7. Zhou X, Otsuji Y, Yoshifuku S, Yuasa T, Zhang H, Takasaki K, Matsukida K, Kisanuki A, Minagoe S, Tei C. Impact of atrial fibrillation on tricuspid and mitral annular dilatation and valvular regurgitation. Circ J. 2002; 66:913–916.
Article8. Najib MQ, Vinales KL, Vittala SS, Challa S, Lee HR, Chaliki HP. Predictors for the development of severe tricuspid regurgitation with anatomically normal valve in patients with atrial fibrillation. Echocardiography. 2012; 29:140–146.
Article9. Yamasaki N, Kondo F, Kubo T, Okawa M, Matsumura Y, Kitaoka H, Yabe T, Furuno T, Doi Y. Severe tricuspid regurgitation in the aged: atrial remodeling associated with long-standing atrial fibrillation. J Cardiol. 2006; 48:315–323.10. Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, Weyman AE. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990; 82:792–797.
Article11. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1–39.e14.12. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010; 23:685–713. quiz 786-813. Fukuda S, Gillinov AM, Song JM, Daimon M, Kongsaerepong V, Thomas JD, Shiota T. Echocardiographic insights into atrial and ventricular mechanisms of functional tricuspid regurgitation. Am Heart J. 2006; 152:1208–1214.14. Singh JP, Evans JC, Levy D, Larson MG, Freed LA, Fuller DL, Lehman B, Benjamin EJ. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study). Am J Cardiol. 1999; 83:897–902.15. Topilsky Y, Nkomo VT, Vatury O, Michelena HI, Letourneau T, Suri RM, Pislaru S, Park S, Mahoney DW, Biner S, Enriquez-Sarano M. Clinical outcome of isolated tricuspid regurgitation. JACC Cardiovasc Imaging. 2014; 7:1185–1194.16. Kim HK, Kim YJ, Park JS, Kim KH, Kim KB, Ahn H, Sohn DW, Oh BH, Park YB, Choi YS. Determinants of the severity of functional tricuspid regurgitation. Am J Cardiol. 2006; 98:236–242.17. Seo HS, Ha JW, Moon JY, Choi EY, Rim SJ, Jang Y, Chung N, Shim WH, Cho SY, Kim SS. Right ventricular remodeling and dysfunction with subsequent annular dilatation and tethering as a mechanism of isolated tricuspid regurgitation. Circ J. 2008; 72:1645–1649.18. Ton-Nu TT, Levine RA, Handschumacher MD, Dorer DJ, Yosefy C, Fan D, Hua L, Jiang L, Hung J. Geometric determinants of functional tricuspid regurgitation: insights from 3-dimensional echocardiography. Circulation. 2006; 114:143–149.19. Spinner EM, Lerakis S, Higginson J, Pernetz M, Howell S, Veledar E, Yoganathan AP. Correlates of tricuspid regurgitation as determined by 3D echocardiography: pulmonary arterial pressure, ventricle geometry, annular dilatation, and papillary muscle displacement. Circ Cardiovasc Imaging. 2012; 5:43–50.20. Hung J. The pathogenesis of functional tricuspid regurgitation. Semin Thorac Cardiovasc Surg. 2010; 22:76–78.21. Fukuda S, Song JM, Gillinov AM, McCarthy PM, Daimon M, Kongsaerepong V, Thomas JD, Shiota T. Tricuspid valve tethering predicts residual tricuspid regurgitation after tricuspid annuloplasty. Circulation. 2005; 111:975–979.22. Mikami T, Kudo T, Sakurai N, Sakamoto S, Tanabe Y, Yasuda H. Mechanisms for development of functional tricuspid regurgitation determined by pulsed Doppler and two-dimensional echocardiography. Am J Cardiol. 1984; 53:160–163.23. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. American Society of Echocardiography. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003; 16:777–802.24. Lancellotti P, Moura L, Pierard LA, Agricola E, Popescu BA, Tribouilloy C, Hagendorff A, Monin JL, Badano L, Zamorano JL. European Association of Echocardiography. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr. 2010; 11:307–332.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tricuspid Regurgitation in Patients with Atrial Septal Defect
- Revisit of Functional Tricuspid Regurgitation; Current Trends in the Diagnosis and Management
- Assessment of Mitral Stenosis by Doppler Echocardiography: Influence of Atrial Fibrillation of Doppler Pressure Half-Time
- Erratum: Correction of the Author's Name. Risk Factors between Patients with Lone and Non-Lone Atrial Fibrillation by Lee SH, et al. (J Korean Med Sci. 2013;28:1174-80.)
- The Relation between Mitral Valve Disease and Atrial Fibrillation
