Tumor-Mimicking Large Vegetation Attached to the Tricuspid Valve without Predisposing Factors: A Case Report on CT and Echocardiographic Findings
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yhchoe@skku.edu
- 2HVSI Imaging Center, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Thoracic and Cardiovascular Surgery, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Division of Infectious Diseases, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 6Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2068719
- DOI: http://doi.org/10.3348/jksr.2015.73.4.269
Abstract
- We report the CT and echocardiographic findings of a tumor-mimicking large vegetation attached to the tricuspid valve (TV) of a 45-year-old man without predisposing factors. Echocardiography revealed a mobile homogeneous echogenic mass attached to the TV. Cardiac CT showed a 4.5 x 2.3 cm irregular low-density mass with scant enhancement in the right ventricle. Based on clinical findings of fever, positive blood culture results for Streptococcus viridans, and pathologic confirmation of the lesion, a diagnosis of infective endocarditis and vegetation was made.
MeSH Terms
Figure
-
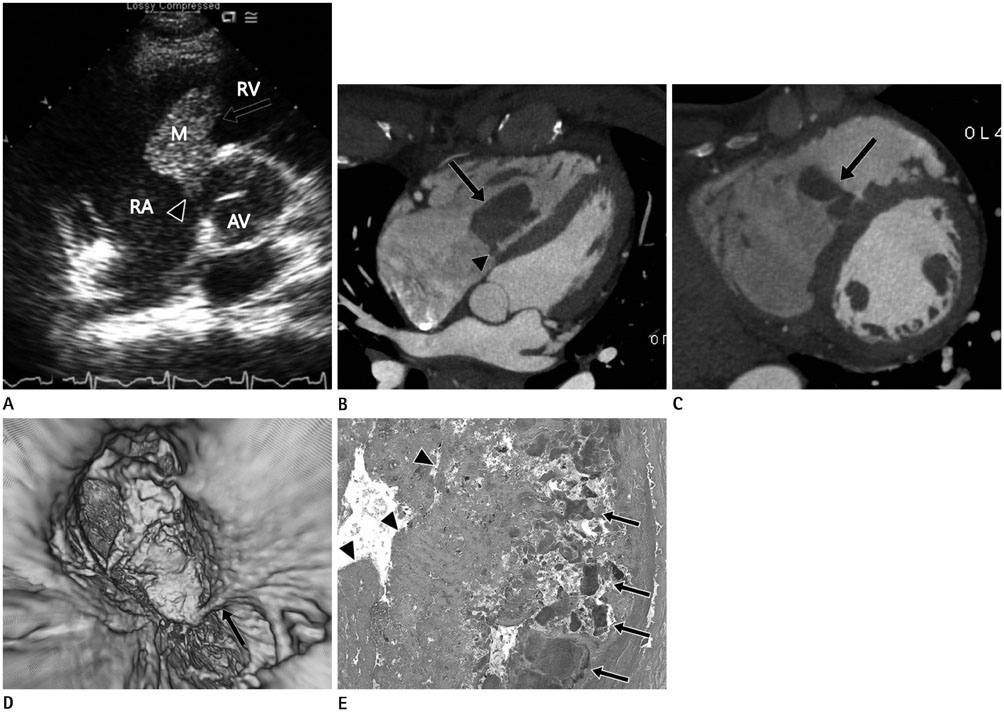
Fig. 1 A 45-year-old man with a mass in the right ventricle. A. Transthoracic echocardiogram revealing a 4.5 × 2.3 cm highly mobile homogeneous echogenic mass (arrow) attached to the tricuspid valve (arrowhead). B, C. Four-chamber (B) and short-axial (C) CT reformatted images showing a 4 cm irregular low-density mass with an attenuation value of 75 HU (arrows in B and C). The mass is seen attached to the tricuspid valve on 4-chamber view (arrowhead in B). D. Virtual endoscopic CT reconstructed image demonstrating attachment of the mass to the tricuspid valve (arrow). E. Photomicrograph revealing multiple bacterial colonies (arrows) intermingled with fibrinopurulent inflammatory exudate (arrowheads) (hematoxylin and eosin stain, magnification × 200). AV = aortic valve, HU = Hounsfield units, M = mass, RA = right atrium, RV = right ventricle
Reference
-
1. Cosson S, Kevorkian JP, Milliez P, Beaufils P, Cohen A. A rare localization in right-sided endocarditis diagnosed by echocardiography: a case report. Cardiovasc Ultrasound. 2003; 1:10.2. Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000; 30:633–638.3. Fellah L, Waignein F, Wittebole X, Coche E. Combined assessment of tricuspid valve endocarditis and pulmonary septic embolism with ECG-gated 40-MDCT of the whole chest. AJR Am J Roentgenol. 2007; 189:W228–W230.4. Uppal KM, Nuño IN, Schwartz DS, Ashton KA, Starnes VA. Isolated right ventricular outflow tract mass presenting as hemoptysis. Ann Thorac Surg. 2000; 70:2158–2159.5. Passen E, Feng Z. Cardiopulmonary manifestations of isolated pulmonary valve infective endocarditis demonstrated with cardiac CT. J Cardiovasc Comput Tomogr. 2015; 04. 08. [Epub]. DOI: 10.1016/j.jcct.2015.03.013.6. Gowda RM, Khan IA, Nair CK, Mehta NJ, Vasavada BC, Sacchi TJ. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am Heart J. 2003; 146:404–410.7. Mazzeffi M, Reich DL, Adams DH, Fischer GW. A mitral valve mass: tumor, thrombus, or vegetation? J Cardiothorac Vasc Anesth. 2011; 25:889–890.8. Grob A, Thuny F, Villacampa C, Flavian A, Gaubert JY, Raoult D, et al. Cardiac multidetector computed tomography in infective endocarditis: a pictorial essay. Insights Imaging. 2014; 5:559–570.9. Martín-Dávila P, Navas E, Fortún J, Moya JL, Cobo J, Pintado V, et al. Analysis of mortality and risk factors associated with native valve endocarditis in drug users: the importance of vegetation size. Am Heart J. 2005; 150:1099–1106.10. Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 2009; 30:2369–2413.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tricuspid Papillary Fibroelastoma Mimicking Tricuspid Vegetation in a Patient with Severe Neutropenia
- A Case of Tricuspid Valve Endocarditis with Vegetation in a Non-Drug Addict without Underlying Cardiac Disease
- The Right Ventricular Myxoma Which Attached to the Tricuspid Valve: Sliding Tricuspid Valvuloplasty
- Isolated Native Valve Endocarditis on Tricuspid Valve: A Case Report
- Transvenous Pacemaker Lead Removal in Pacemaker Lead Endocarditis with Large Vegetations: A Report of Two Cases
