Antihypertensive drug combinations
- Affiliations
-
- 1Department of Medicine/Cardiology, Cheil General Hospital, Kwandong University College of Medicine, Seoul, Korea. mdparkjb@gmail.com
- KMID: 2064882
- DOI: http://doi.org/10.5124/jkma.2014.57.3.253
Abstract
- Hypertension has a diverse pathophysiology. Theoretically, one drug is not sufficient to control high blood pressure (BP) in most hypertension. Therefore, the combination of two or more drugs with different mechanisms is needed to meet the target BP. In setting the target BP, a low-dose combination of two drugs with different mechanisms has greater efficacy and safety than a higher dose of one drug. Recent clinical trials and hypertension guidelines from different parts of the world report that the combination of renin-angiotensin system inhibitors with calcium channel antagonists or diuretics is generally recommended but combinations including beta-blockers, rarely so. However, if even a combination of three drugs all with different mechanisms, each at full dose does not control the BP, then a beta-blocker and/or other antihypertensive drug should be considered. Rarely, an interventional procedure such as renal sympathetic denervation has been applied, but evidence supporting such therapies remains limited.
Keyword
MeSH Terms
Figure
-
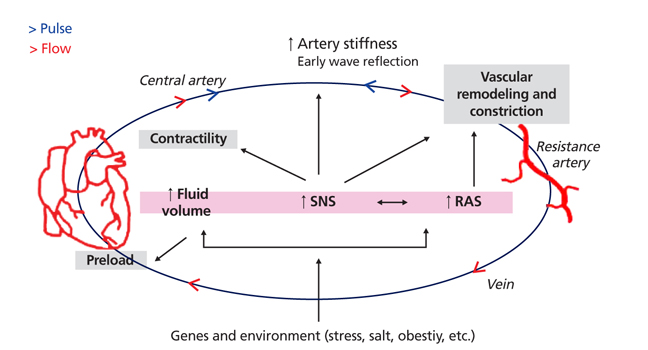
Figure 1 A diverse pathophysiology of hypertension development. Hemodynamic and neuro-hormonal changes contribute blood pressure elevation and vascular alterations. SNS, sympathetic nerve system; RAS, renin angiotensin system.
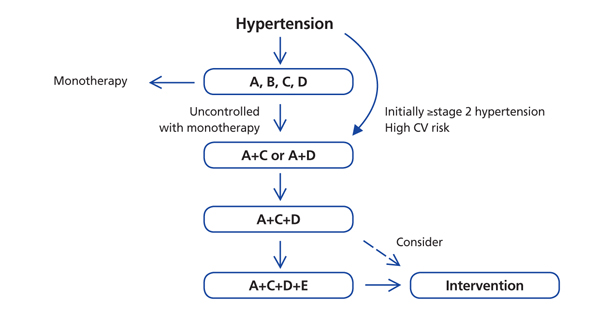
Figure 2 Monotherapy or drug combination strategies to achieve target blood pressure. Moving from monotherapy to quadruple therapy and with interventional approach as an option should be done whenever blood pressure target is not achieved. CV, cardiovascular. A, angiotensin converting enzyme inhibitor or angiotensin receptor blocker; B, beta-blockers; C, calcium channel blocker; D, thiazide or thiazide-like diuretic; E, et cetera (alpha- or beta-blocker, spinolactone, loop diuretic and others).
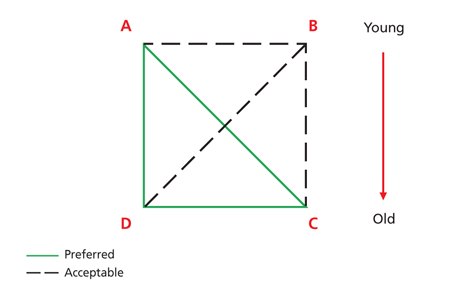
Figure 3 Preferred, and acceptable combinations of antihypertensive drugs. A, angiotensin converting enzyme inhibitor or angiotensin receptor blocker; B, beta-blocker; C, calcium channel blocker; D, thiazide or thiazide-like diuretic. Modified from Korean Society of Hypertension. 2013 Guideline on hypertension by Korean Society of Hypertension [Internet]. Seoul: Korean Society of Hypertension; 2013 [1].
Reference
-
1. Korean Society of Hypertension. 2013 Guideline on hyperten-sion by Korean Society of Hypertension [Internet]. Seoul: Korean Society of Hypertension;2013. cited 2014 Feb 24. Available from: http://www.koreanhypertension.org.2. Materson BJ, Reda DJ, Cushman WC, Massie BM, Freis ED, Kochar MS, Hamburger RJ, Fye C, Lakshman R, Gottdiener J, Ramirez EA, William G. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. Single-drug therapy for hypertension in men: a comparison of six antihypertensive agents with placebo. N Engl J Med. 1993; 328:914–921.
Article3. Milani RV. Reaching for aggressive blood pressure goals: role of angiotensin receptor blockade in combination therapy. Am J Manag Care. 2005; 11:7 Suppl. S220–S227.4. Düsing R. Optimizing blood pressure control through the use of fixed combinations. Vasc Health Risk Manag. 2010; 6:321–325.
Article5. Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. Am J Med. 2009; 122:290–300.
Article6. Weir MR. The rationale for combination versus single-entity therapy in hypertension. Am J Hypertens. 1998; 11:163S–169S.
Article7. ONTARGET Investigators. Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, Schumacher H, Dagenais G, Sleight P, Anderson C. Telmisartan, ramipril, or both in patients at high risk for vascu-lar events. N Engl J Med. 2008; 358:1547–1559.
Article8. Vanhoutte PM, Gao Y. Beta blockers, nitric oxide, and cardiovascular disease. Curr Opin Pharmacol. 2013; 13:265–273.
Article9. National Institute for Health and Care Excellence. Hypertension: clinical management of primary hypertension in adults [Internet]. London: National Institute for Health and Care Excellence;2006. cited 2013 Feb 24. Available from: http://guidance.nice.org.uk/CG127.10. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F, Redon J, Dominiczak A, Narkiewicz K, Nilsson PM, Burnier M, Viigimaa M, Ambrosioni E, Caufield M, Coca A, Olsen MH, Schmieder RE, Tsioufis C, van de Borne P, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Clement DL, Coca A, Gillebert TC, Tendera M, Rosei EA, Ambrosioni E, Anker SD, Bauersachs J, Hitij JB, Caulfield M, De Buyzere M, De Geest S, Derumeaux GA, Erdine S, Farsang C, Funck-Brentano C, Gerc V, Germano G, Gielen S, Haller H, Hoes AW, Jordan J, Kahan T, Komajda M, Lovic D, Mahrholdt H, Olsen MH, Ostergren J, Parati G, Perk J, Polonia J, Popescu BA, Reiner Z, Ryden L, Sirenko Y, Stanton A, Struijker-Boudier H, Tsioufis C, van de Borne P, Vlachopoulos C, Volpe M, Wood DA. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013; 34:2159–2219.11. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014; 311:507–520.
Article12. Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG, Flack JM, Carter BL, Materson BJ, Ram CV, Cohen DL, Cadet JC, Jean-Charles RR, Taler S, Kountz D, Townsend R, Chalmers J, Ramirez AJ, Bakris GL, Wang J, Schutte AE, Bisognano JD, Touyz RM, Sica D, Harrap SB. Clinical practice guidelines for the management of hypertension in the community a statement by the american society of hypertension and the international society of hypertension. J Hypertens. 2014; 32:3–15.
Article13. Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O'Brien E, Ostergren J. ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 2005; 366:895–906.
Article14. Jamerson K, Weber MA, Bakris GL, Dahlof B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ. ACCOMPLISH Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008; 359:2417–2428.
Article15. Beckett NS, Peters R, Fletcher AE, Staessen JA, Liu L, Dumitrascu D, Stoyanovsky V, Antikainen RL, Nikitin Y, Anderson C, Belhani A, Forette F, Rajkumar C, Thijs L, Banya W, Bulpitt CJ. HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008; 358:1887–1898.
Article16. Patel A; ADVANCE Collaborative Group, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, Harrap S, Poulter N, Marre M, Cooper M, Glasziou P, Grobbee DE, Hamet P, Heller S, Liu LS, Mancia G, Mogensen CE, Pan CY, Rodgers A, Williams B. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007; 370:829–840.
Article17. Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B, Zanchetti A. VALUE trial group. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet. 2004; 363:2022–2031.
Article18. Messerli FH, Bangalore S, Julius S. Risk/benefit assessment of beta-blockers and diuretics precludes their use for first-line therapy in hypertension. Circulation. 2008; 117:2706–2715.
Article19. Calhoun DA, Lacourciere Y, Chiang YT, Glazer RD. Triple antihypertensive therapy with amlodipine, valsartan, and hydrochlorothiazide: a randomized clinical trial. Hypertension. 2009; 54:32–39.
Article20. Kereiakes DJ, Chrysant SG, Izzo JL Jr, Littlejohn T 3rd, Oparil S, Melino M, Lee J, Fernandez V, Heyrman R. Long-term efficacy and safety of triple-combination therapy with olmesartan medoxomil and amlodipine besylate and hydrochlorothiazide for hypertension. J Clin Hypertens (Greenwich). 2012; 14:149–157.
Article21. Gaddam KK, Nishizaka MK, Pratt-Ubunama MN, Pimenta E, Aban I, Oparil S, Calhoun DA. Characterization of resistant hypertension: association between resistant hypertension, aldosterone, and persistent intravascular volume expansion. Arch Intern Med. 2008; 168:1159–1564.
Article22. Chapman N, Chang CL, Dahlof B, Sever PS, Wedel H, Poulter NR. ASCOT Investigators. Effect of doxazosin gastrointestinal therapeutic system as third-line antihypertensive therapy on blood pressure and lipids in the Anglo-Scandinavian Cardiac Outcomes Trial. Circulation. 2008; 118:42–48.
Article23. Symplicity HTN-2 Investigators. Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Böhm M. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010; 376:1903–1909.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Response surface analyses of antihypertensive effects of angiotensin receptor blockers and amlodipine or hydrochlorothiazide combination therapy in patients with essential hypertension
- Sympathetic Ophthalmia after Ocular Wasp Sting
- Is amlodipine more cardioprotective than other antihypertensive drug classes?
- Antihypertensive and antihyperglycemic effects of combinations of losartan with metformin and/or glibenclamide in desoxycorticosterone acetate and streptozotocin‑induced hypertensive diabetic rats
- Pharmacogenomics in Drug Discovery and Development
