Clipping of Incidental Aneurysm of Middle Cerebral Artery Through Small Temporal Craniotomy and Linear Skin Incision
- Affiliations
-
- 1Department Neurosurgery, Gwangju Christian Hospital, Gwangju, Korea. nsmh1@hanmail.net
- KMID: 2055282
- DOI: http://doi.org/10.7461/jcen.2014.16.1.32
Abstract
- The authors introduced a new approach for clipping of the incidental aneurysm of the middle cerebral artery (MCA) and reported the clinical results. We retrospectively reviewed 26 patients with 27 incidental MCA aneurysms who were treated from January 2010 to December 2012. All clippings were performed through a small temporal craniotomy and linear skin incision. Follow-up imaging showed complete occlusion of 26 aneurysms (96.3%), residual neck in one (3.7%). In one case, residual neck of the aneurysm did not grow on serial follow up. In one of 26 cases (3.8%), approach-related complication was retraction injury of the temporal cortex. Two patients developed postoperative infarction on the MCA territories due to vasospasm and on the cerebellum due to unknown causes. These were not approach-related complications. Operation time was 95 min-250 min (mean 143 min). There were no complications of temporal muscle atrophy, scar deformity, paresthesia, or pain around the scalp incision and frontalis palsy. This approach offers good surgical possibilities and little approach related morbidity in the clipping of incidental MCA aneurysms.
MeSH Terms
Figure
-
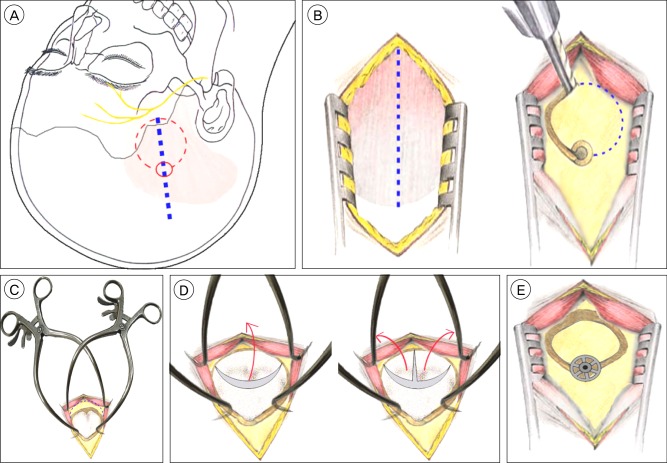
Fig. 1 A-E. Schematic drawings illustrating the operative procedure. (A) Scalp incision (blue-dashed line) and craniotomy (red-dashed line), frontal branch of the facial nerve (yellow line) (B) Right: temporalis muscle incision (blue-dotted line) Left: one burr hole and craniotomy (blue dotted line) (C) Retraction using two Gelpi retractors and more resection of the sphenoid ridge (blue-dotted line). One side of the Gelpi retractors is located to the bony margin of craniotomy and the other side to the temporalis muscle. (D) Incision of dura mater: a curved and inverted T-shaped fashion The red arrow indicates that the free dural flap is reflected anteriorly. (E) Fixation of the bone flap by a titanium Craniofix miniplate.
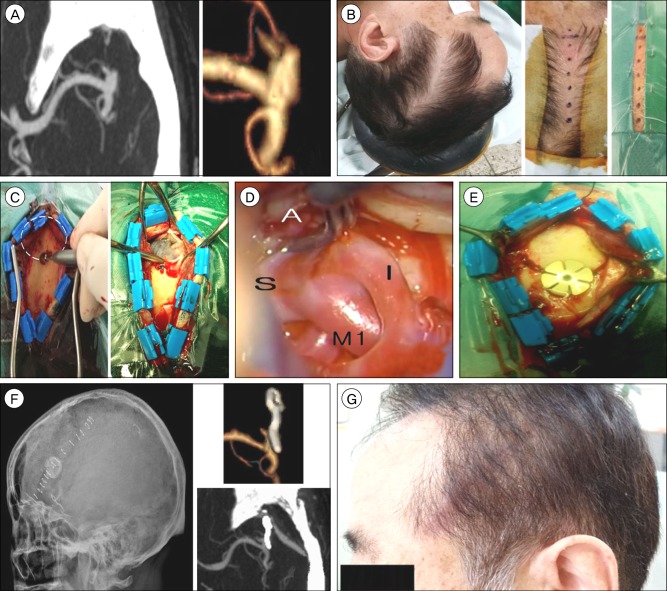
Fig. 2 A-G. Case report: preoperative, intraoperative, postoperative findings. (A) Preoperative computed tomography angiography shows a left middle cerebral artery (MCA) bifurcation aneurysm: unruptured and a saccular type measuring 6×4mm in size. (B) Position and scalp incision (dotted line). (C) Left: One burr hole and craniotomy (white-dashed line). Right: C-shaped fashion dural incision and free dural flap is reflected anteriorly and exposure of the distal sylvian fissure and posterior part of the inferior frontal gyrus and superior temporal gyrus. (D) Intraoperative clipping of an aneurysm (M: M1 trunk, S: superior trunk of M2, I: inferior trunk of M2, A: aneurysm). (E) Fixation of the bone flap by a titanium Craniofix miniplate. (F) Postoperative radiologic findings: skull X-ray lateral view and computed tomography angiography. (G) Photography of patient postoperatively two weeks later.
Reference
-
1. Johnson AK, Heiferman DM, Lopes DK. Stent-assisted embolization of 100 middle cerebral artery aneurysm. J Neurosurg. 2013; 5. 118(5):950–955. PMID: 23394339.2. Cha KC, Hong SC, Kim JS. Comparison between lateral supraorbital approach and pterional approach in the surgical treatment of unruptured intracranial aneurysms. J Korean Neurosurg Soc. 2012; 6. 51(6):334–337. PMID: 22949961.
Article3. Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, et al. The minipterional craniotomy: Technical description and anatomic assessment. Neurosurgery. 2007; 11. 61(5 Suppl 2):256–264. discussion 264-5. PMID: 18091240.
Article4. Figueiredo EG, Deshmukh V, Nakaji P, Deshmukh P, Crusius MU, Crawford N, et al. An anatomical evaluation of the mini-supraorbital approach and comparison with standard craniotomies. Neurosurgery. 2006; 10. 59(4 Suppl 2):ONS212–ONS220. discussion ONS220. PMID: 17041490.
Article5. Hernesniemi J, Ishii K, Niemela M, Smrcka M, Kivipelto L, Fujiki M, et al. Lateral supraorbital approach as an alternative to the classical pterional approach. Acta Neurochir Suppl. 2005; 94:17–21. PMID: 16060236.
Article6. McLaughlin N, Cutler A, Martin NA. Technical nuances of temporal muscle dissection and reconstruction for the pterional keyhole craniotomy: Technical note. J Neurosurg. 2013; 2. 118(2):309–314. PMID: 23140151.7. Park J, Hamm IS. Cortical osteotomy technique for mobilizing the temporal muscle in pterional craniotomies. Technical note. J Neurosurg. 2005; 1. 102(1):174–178. PMID: 15658112.8. Tummala RP, Başkaya MK, Heros RC. Contemporary management of incidental intracranial aneurysms. Neurosurg Focus. 2005; 1. 18(1):e9. PMID: 15669803.
Article9. Regli L, Dehdashti AR, Uske A, de Tribolet N. Endovascular coiling compared with surgical clipping for the treatment of unruptured middle cerebral artery aneurysms: An update. Acta Neurochir Suppl. 2002; 82:41–46. PMID: 12378989.
Article10. Heros RC. The supraorbital "keyhole" approach. J Neurosurg. 2011; 3. 114(3):850–851. discussion 851. PMID: 21029040.11. Spetzler RF, Lee KS. Reconstruction of the temporalis muscle for the pterional craniotomy: Technical note. J Neurosurg. 1990; 10. 73(4):636–637. PMID: 2398396.12. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms: Concept and technique. Surg Neurol. 1998; 5. 49(5):481–489. discussion 489-90. PMID: 9586924.
Article13. Yasargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol. 1975; 1. 3(1):7–14. PMID: 1111150.14. Yaşargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg. 1987; 9. 67(3):463–466. PMID: 3612281.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified Clipping on Broad Neck Aneurysm of Middle Cerebral Artery
- Surgical Experiences of the Ruptured Giant Middle Cerebral Artery Aneurysm(2 Cases)
- Emergency In Situ Bypass during Middle Cerebral Artery Aneurysm Surgery: Middle Cerebral Artery-Superficial Temporal Artery Interposition Graft-Middle Cerebral Artery Anastomosis
- Middle Cerebral Artery Aneurysm in a Premature Neonate
- Superficial Temporal Artery-Sparing Mini-Pterional Approach for Cerebral Aneurysm Surgery
