Dyspareunia Caused by Pelvis Malunion
- Affiliations
-
- 1Department of Orthopedic Surgery, Daejeon St. Mary's Hospital, The Catholic University of Korea, College of Medicine, Daejeon, Korea. weonkim@hotmail.com
- KMID: 2054162
- DOI: http://doi.org/10.5371/hp.2014.26.1.45
Abstract
- In unstable pelvic ring injury, if there is damage to both the anterior and posterior, both anterior and posterior fixation will be needed in order to stabilze the pelvic ring. A female patient complained of dyspareunia due to malunion and additional bone bridge at the inferior ramus of the pelvis. She should have undergone both anterior and posterior fixation, but had undergone anterior fixation only. We report on a patient who was treated successfully with resection of additional bone bridge, scar tissue and adhesive band around the vagina.
Figure
-
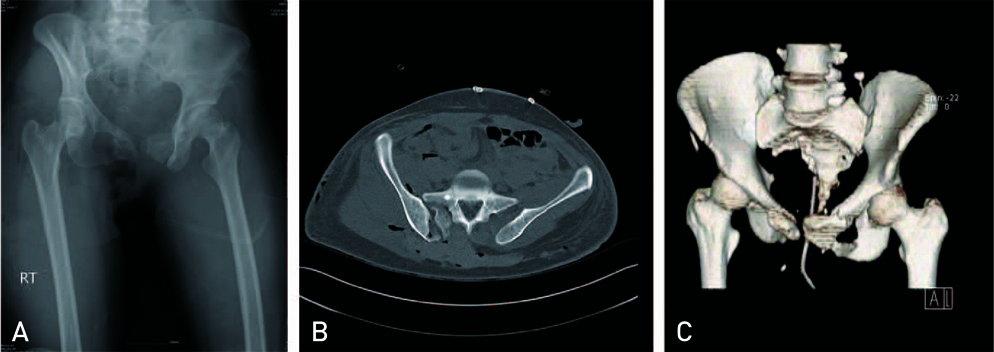
Fig. 1 (A) Initial pelvis anteroposterior radiograph, (B) comuputerized tomography image, (C) and 3-dimensional reconstructed image show both rami fracture and right sacro-iliac joint disruption (Tile type C [AO/OTA type C]).

Fig. 2 On the situation of extensive soft tissue damage around sacrum, despite Tile type C (AO/OTA type C), posterior stabilization did not be performed, but the reduction and anterior stabilization were achieved by external fixator.
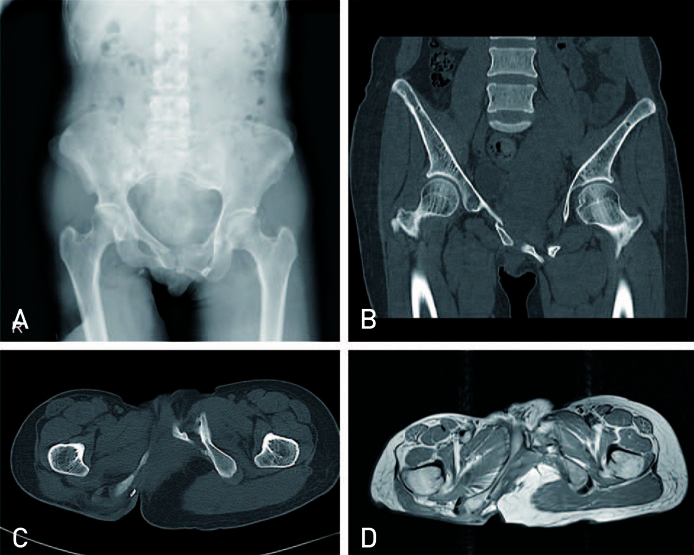
Fig. 3 (A) After 6 years of operation. Plain radiograph, (B) coronal image, (C) and axial image of computed tomography scan (D) show the superior migration of right ilium and the formation of bony bridge at left inferior ramus. Consequently, vaginal wall compressed by the protruded bony bridge is seen in axial image of T2 weighted magnetic resonance imaging.
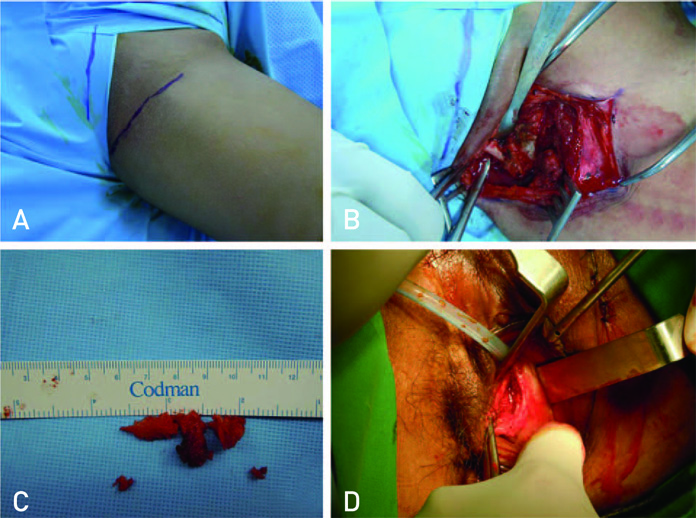
Fig. 4 (A) Gross photo shows the incision line for inguinal approach. (B) The protruded bony bridge was exposed through inguinal approach. (C) Excised fragments which were consisted of the bony bridge. (D) The excision of constricting band formed by scar tissue was performed using trans-vaginal approach.
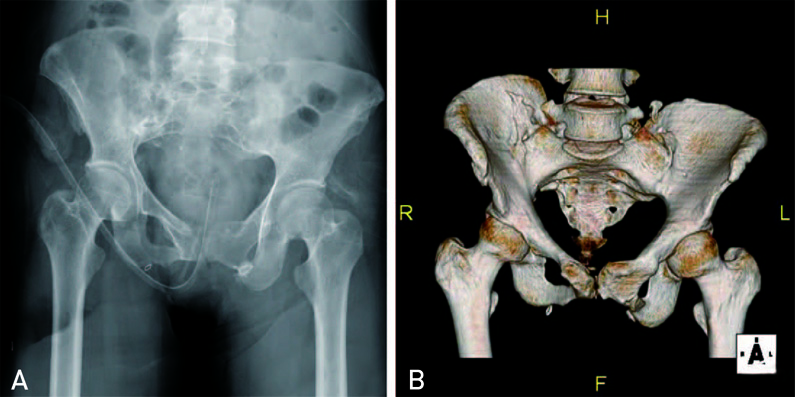
Fig. 5 Plain radiograph (A) and 3-dimensional computed tomography image (B) show the finding that the protruded bony bridge was excised. R: right, L: left, H: head, F: feet
Reference
-
1. Gänsslen A, Pohlemann T, Paul C, Lobenhoffer P, Tscherne H. Epidemiology of pelvic ring injuries. Injury. 1996; 27:Suppl 1. S-A13–S-A20.
Article2. Simonian PT, Routt ML Jr. Biomechanics of pelvic fixation. Orthop Clin North Am. 1997; 28:351–367.
Article3. Dujardin FH, Roussignol X, Hossenbaccus M, Thomine JM. Experimental study of the sacroiliac joint micromotion in pelvic disruption. J Orthop Trauma. 2002; 16:99–103.
Article4. Papadopoulos IN, Kanakaris N, Bonovas S, et al. Auditing 655 fatalities with pelvic fractures by autopsy as a basis to evaluate trauma care. J Am Coll Surg. 2006; 203:30–43.
Article5. Matewski D, Szymkowiak E, Bilinski P. Analysis of management of patients with multiple injuries of the locomotor system. Int Orthop. 2008; 32:753–758.
Article6. Riska EB, von Bonsdorf H, Hakkinen S, Jaroma H, Kiviluoto O, Paavilainen T. External fixation of unstable pelvic fractures. Int Orthop. 1979; 3:183–188.
Article7. Schweitzer G. Open reduction and internal fixation of vertical shear pelvic fractures. J Trauma. 1987; 27:1308.8. Kellam JF, McMurtry RY, Paley D, Tile M. The unstable pelvic fracture. Operative treatment. Orthop Clin North Am. 1987; 18:25–41.9. Berg EE, Chebuhar C, Bell RM. Pelvic trauma imaging: a blinded comparison of computed tomography and roentgenograms. J Trauma. 1996; 41:994–998.10. Vallier HA, Cureton BA, Schubeck D. Pregnancy outcomes after pelvic ring injury. J Orthop Trauma. 2012; 26:302–307.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Malunion and Nonunion after Pelvic Bone Fracture
- Surgical Correction of Pelvic Malunion and Nonunion
- Diagnosis and Treatment of Dyspareunia
- The effect of isoflavone on vaginal dryness and dyspareunia in postmenopausal symptoms: a systematic review and meta-analysis
- A Correction of Malunion or Deformity in the Lower Extremity
