Paralabral Cysts and Their Correlation with Acetabular Disorder
- Affiliations
-
- 1Department of Orthopedic Surgery, Research Institute for Medical Science, Chungnam National University School of Medicine, Daejeon, Korea. dshwang@cnu.ac.kr
- KMID: 2054137
- DOI: http://doi.org/10.5371/hp.2012.24.3.231
Abstract
- PURPOSE
To evaluate the correlation between MRI findings and hip joint lesions evaluated by arthroscopy in patients affected by paralabral cyst.
MATERIALS AND METHODS
Of patients treated by hip arthroscopy from Jan 1996 to Mar 2010, 17 cases symptomatic of paralabral cyst as observed by preoperative MRI were analyzed. The presence of an acetabular labrum tear, and the location and size of the cyst were evaluated using both preoperative MRI and intraoperative arthroscopy. Visual analogue scale (VAS), modified Harris hip scale, and Hip outcome score results were compared as determined by the two assessment methods.
RESULTS
According to the MRI findings, the locations of the cysts included 5 cases in the anterosuperior, 2 anterior, 4 anteroinferior, 2 posterosuperior and 4 posteroinferior. The mean size of all cysts was 25.1x12.5x13.8 mm3. Postoperatively, the mean VAS score for all patients improved from 7.7 to 1.5, their modified Harris hip score improved from 58.8 to 90.7, and their Hip outcome score improved from 54 to 93.5.
CONCLUSION
Painful paralabral cyst was mainly associated with an acetabular labral tear and we concluded that observation of paralabral cyst upon preoperative MRI provided indirect evidence of proximal acetabular labral pathology.
Keyword
MeSH Terms
Figure
-
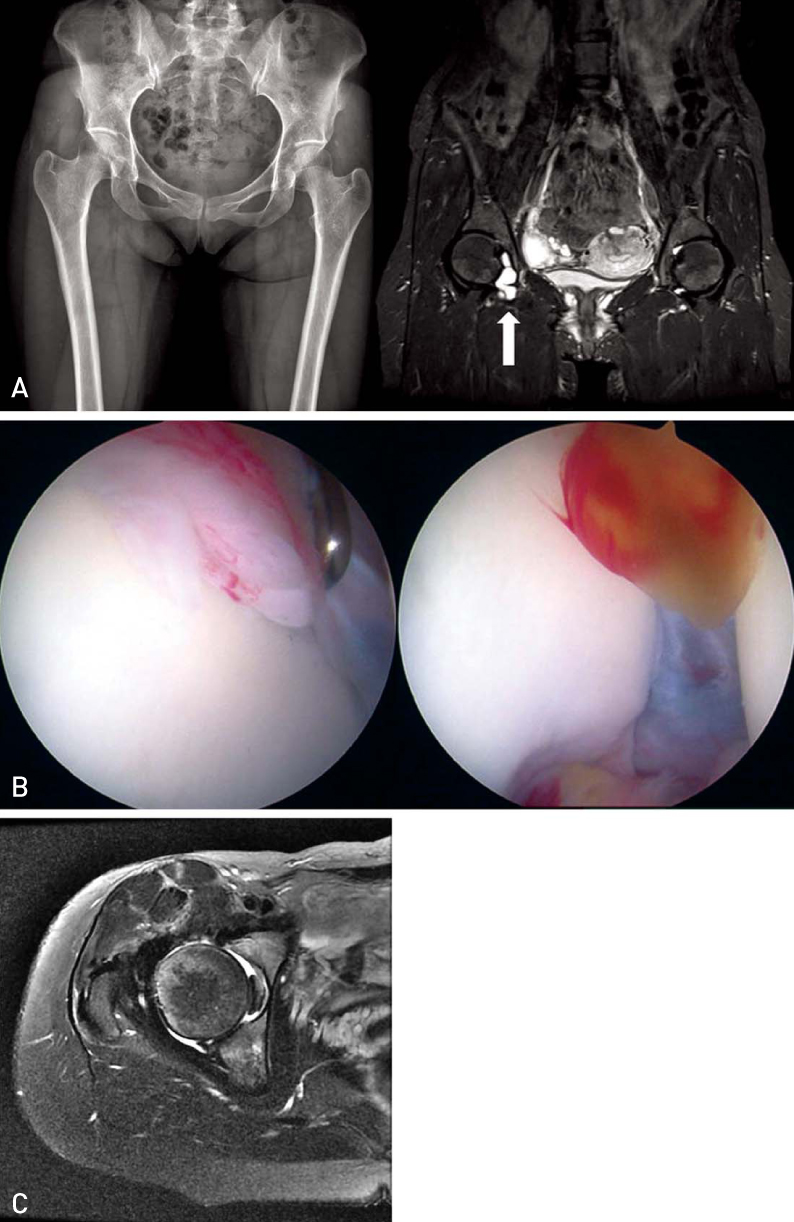
Fig. 1 (A) Preoperative plain radiographs & MRI shows coxa profunda, mild ischial spine sign, and cyst at 3-5 o'clock (arrow). (B) Arthroscopic finding shows labral tear associated paralabral cyst. (C) Postoperative F/U MRI at 2 months shows disappearance of cyst.

Fig. 2 45 years-old female with Rt buttock pain and radiating to leg. (A) Plain radiograph shows the prominent acetabular rim. (B) In MRI, cyst exist from posterior to posteroinferior of the hip joint and multinodular cysts situated along the sciatic nerve (arrows). (C) Arthroscopic finding shows cyst (C) around sciatic nerve and opening to joint (arrow). (D) Extraarticular cyst have been nearly disappeared at POD 22months on MRI. But, cysts around acetabulum was still existed.
Reference
-
1. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R. Acetabular labral tears: evaluation with MR arthrography. Radiology. 1996. 200:231–235.
Article2. Sherman PM, Matchette MW, Sanders TG, Parsons TW. Acetabular paralabral cyst: an uncommon cause of sciatica. Skeletal Radiol. 2003. 32:90–94.
Article3. Magee T, Hinson G. Association of paralabral cysts with acetabular disorders. AJR Am J Roentgenol. 2000. 174:1381–1384.
Article4. Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976. (119):39–47.5. Weinstein SL. Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop Relat Res. 1987. (225):62–76.
Article6. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002. 84:556–560.
Article7. Tannast M, Siebenrock KA. Conventional radiographs to assess femoroacetabular impingement. Instr Course Lect. 2009. 58:203–212.8. Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999. 81:281–288.9. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis--what the radiologist should know. AJR Am J Roentgenol. 2007. 188:1540–1552.
Article10. Kim PS, Hwang DS, Kang C, Lee JB, Lee WW, Han SC. Arthroscopic treatment of femoroacetabular impingement in young taekwondo players. J Korean Orthop Assoc. 2011. 46:303–311.
Article11. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004. (418):67–73.12. Glick JM, Sampson TG, Gordon RB, Behr JT, Schmidt E. Hip arthroscopy by the lateral approach. Arthroscopy. 1987. 3:4–12.
Article13. Ide T, Akamatsu N, Nakajima I. Arthroscopic surgery of the hip joint. Arthroscopy. 1991. 7:204–211.
Article14. Philippon M, Schenker M, Briggs K, Kuppersmith D. Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports Traumatol Arthrosc. 2007. 15:908–914.
Article15. Steiner E, Steinbach LS, Schnarkowski P, Tirman PF, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am. 1996. 34:395–425. xi–xii.16. Haller J, Resnick D, Greenway G, et al. Juxtaacetabular ganglionic (or synovial) cysts: CT and MR features. J Comput Assist Tomogr. 1989. 13:976–983.17. Tyson LL, Daughters TC Jr, Ryu RK, Crues JV 3rd. MRI appearance of meniscal cysts. Skeletal Radiol. 1995. 24:421–424.
Article18. Schnarkowski P, Steinbach LS, Tirman PF, Peterfy CG, Genant HK. Magnetic resonance imaging of labral cysts of the hip. Skeletal Radiol. 1996. 25:733–737.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acetabular Paralabral Cyst as a Rare Cause of Obturator Neuropathy: A Case Report
- Arthroscopic Decompression of an Inferior Paralabral Cyst of the Shoulder in an Elderly Patient: A Case Report
- Multidirectional Instability Accompanying an Inferior Labral Cyst
- Paralabral Cyst of the Hip Compressing Common Femoral Vein Treated with Sono-guided Cyst Aspiration Followed by Arthroscopic Labral Debridement: A Case Report
- Type 2 Superior Labral Anterior to Posterior Lesion-Related Paralabral Cyst Causing Isolated Infraspinatus Paralysis: Two Case Reports
