Five Treatment Models of Dysplastic OA by the RAO
- Affiliations
-
- 1Daegu Health College University Hospital, Daegu, Korea. cskang@empal.com
- KMID: 2054130
- DOI: http://doi.org/10.5371/hp.2012.24.3.165
Abstract
- No abstract available.
Figure
-
Fig. 1 Adapted from Ninomiya, Tagawa JBJS. 1984;65A:430-6.
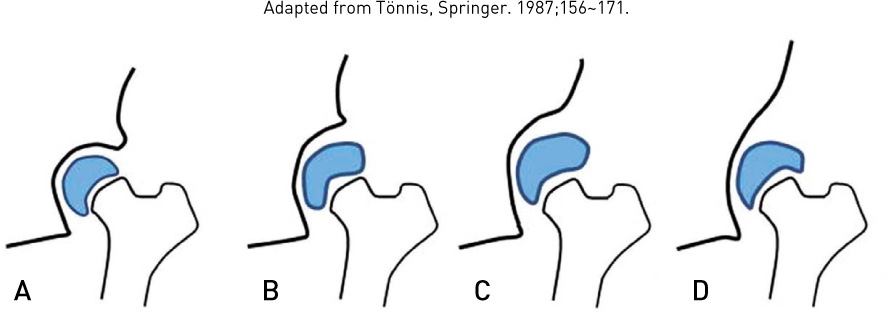
Fig. 2 Drawings illustrating the grades of congruity of the hip joint (adapted from Bauer and Kerschbaumer). (A) Grade 1, (B) Grade 2, (C) Grade 3, (D) Grade 4.

Fig. 3 The resultant force acting on the hip joint in inpotal Monopodal stance phase.

Fig. 4 (A) CE: 8°ROA: 30°, (B) PO CE: 45°ROA: Horizontal, (C) 2007. 9 RAO 23ys (80ys).
Fig. 5 (A) ROA: 30°, CEA: 0°, (B) lateralized acetabulum (thick medial wall, shallow acetabular socket), (C) Do not cut through the Kohlers line, (D) Post op figure.

Fig. 6 (A) CE: 8°, (B) CE: 45°, ROA: reversed, medial shift, (C) 39ys PO 21y.
Fig. 7 (A) Pre op bilateral dysplatic hip, (B) Post op 22ys changed CEA. ROA mealige (22Y).

Fig. 8 (A) CE: -10°, ROA: 35°, (B) Curette out of bone, (C) CE: 45°, ROA: 0°. amount of medialization: 20 mm (2 cm).
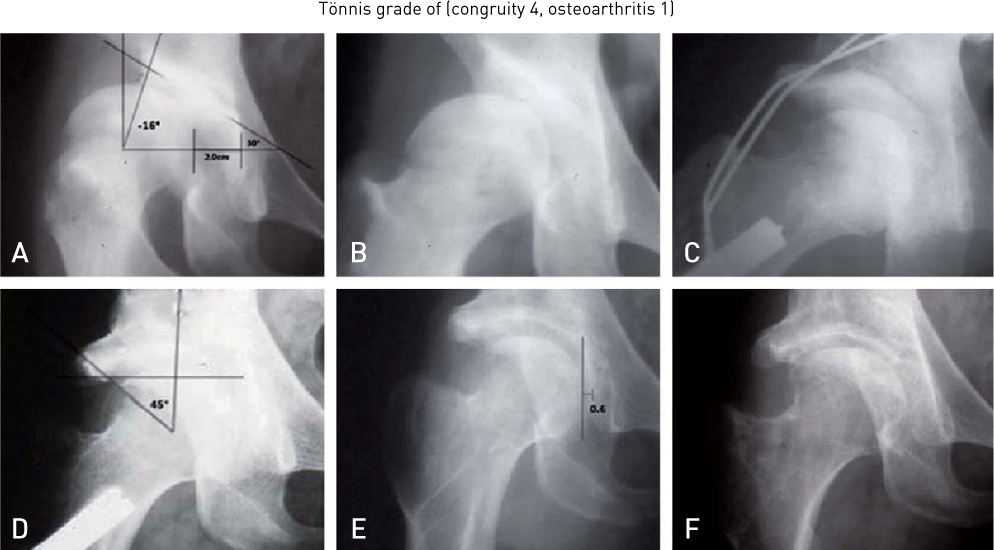
Fig. 9 (A) CE: -16°(reversed), ROA: 30°, (B) IR & Reduction, (C) RAO, (D) CE: 45°, ROA: 0°, (E) Post op 10ys, (F) Post op 25ys.

Fig. 10 Focal cartilage defect of the femoral head (Modification of Marvin E. Steinberg. The hip and Its Disorders, W. B. Saunders company, 1991:9.53).
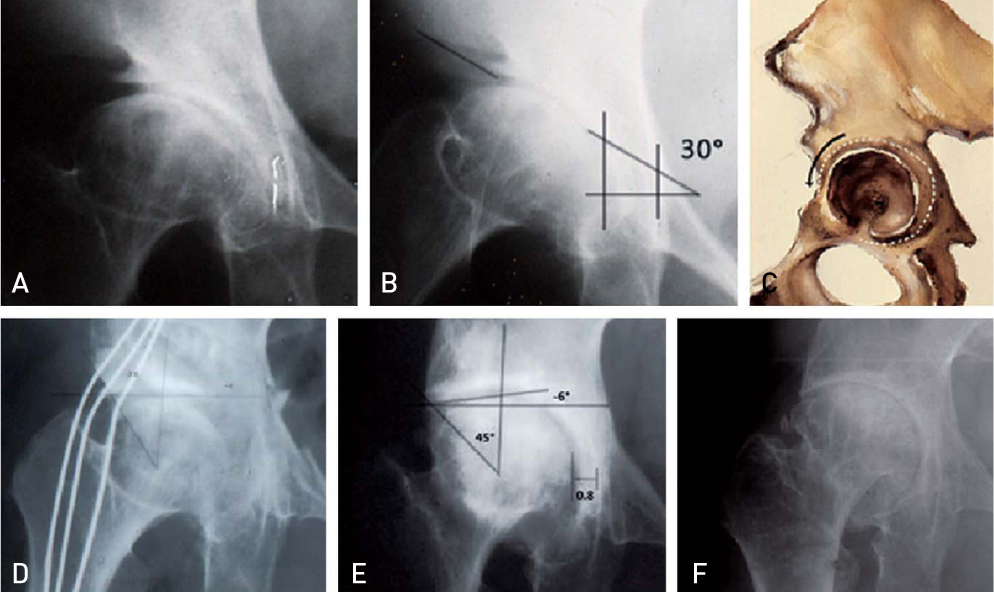
Fig. 11 (A) CE: 10°, multiple columnar head cysts, (B) ROA: 30°, (C) Minimal lateral over rotation and 10 mm anterior rotation, (D) Post op, (E) CE: 45°ROA: +6°, (F) RAO 22ys (2009. 11): multiple head cysts.

Fig. 12 (A) CE; 10°RAO 30°, (B) curtain, floor osteophytes, (C) CE: 45°, (D) Post op 15ys, reversed ROA, medial shift.
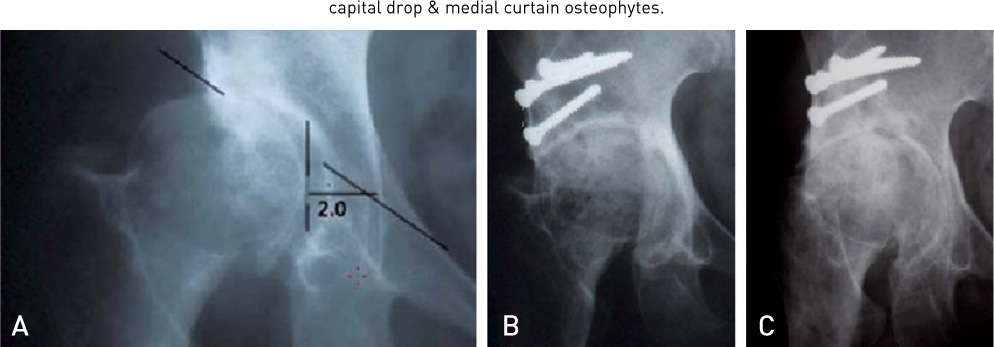
Fig. 13 (A) head cysts, capital drop, floor osteophytes, (B) Post op, ROA reversed; 35°CE; 45°, (C) Post op 20ys(87ys).
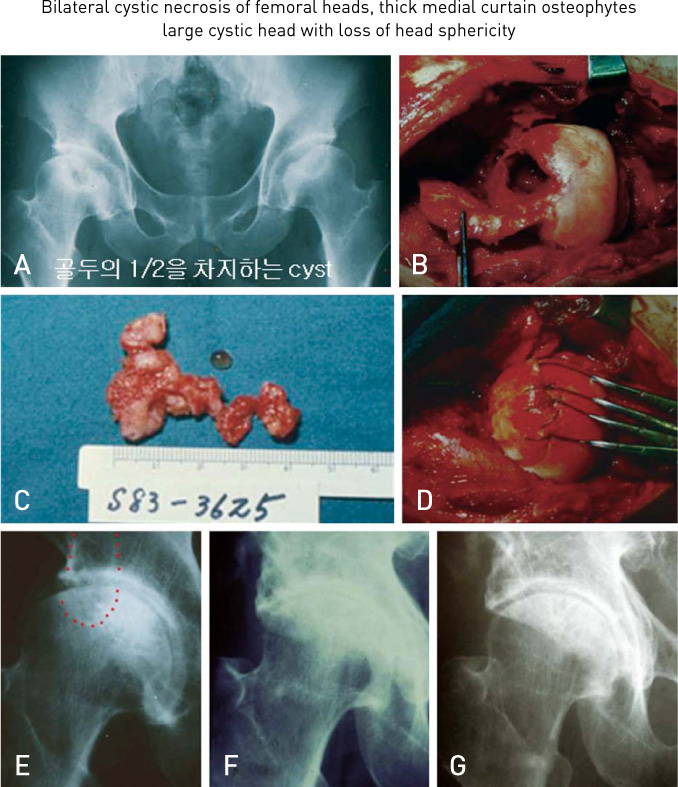
Fig. 14 Bilateral cystic necrosis. (A) A cystic lesion occupies 1/2 of head, (B) Open head window, (C) gross specimem: fibromucoid tissue. (D) After autogenouse cancellous bone graft, catilage suture with 3.0 vicril, expecting Osteoinduction, Osteoconduction. (E) 16ys later operation of curettage head cyst and fill-up autogenous bone graft, Early radiolund cystic kissing lesion lesions in lateral edge acetabulum and femoral head. (F) Performed RAO on R hip for the cystic lesion of the Acetabulum (current & BG). (G) post op 10ys.

Fig. 15 (A) coalesent cysitic necrosis in femoral head, (B) MRI.
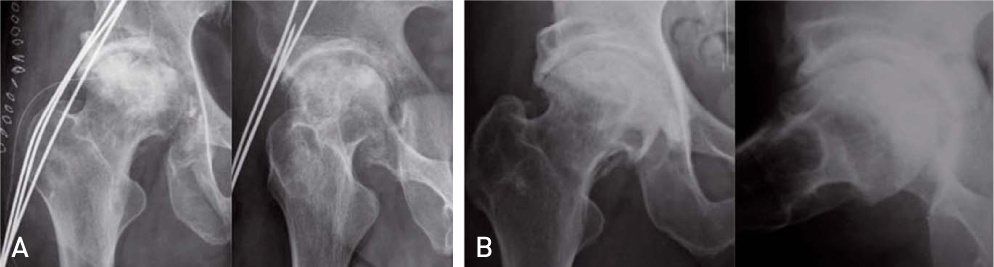
Fig. 16 (A) by the over rotation of Actabulum. We can get the full containment and coverage of femoral head and adequet medilaization (OP 2001. 12), (B) PO 5ys. (53ys. 2006).

Fig. 17 2011. 3. F/U 10y. 58ys. He is very active Golfer, Cellist.
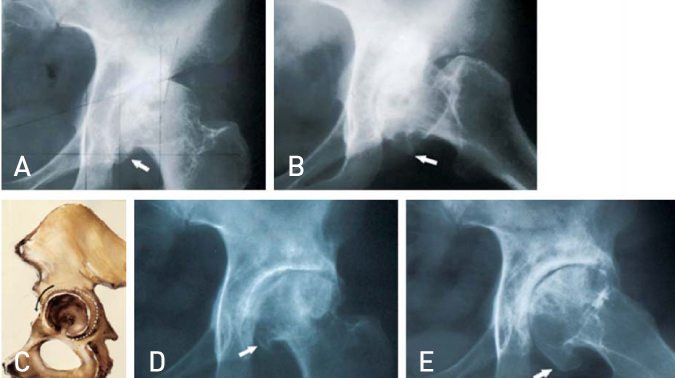
Fig. 18 (A), (B) head cysts, capital drop, curtain osteophytes, (C) illustration of adequete lateral rotation and 10 mm anterior rotation (D) Post op 5ys.

Fig. 19 (A), (B), (C), (D), (E), (F) multi-columnar cysts are persisted longer period 14ys.

Fig. 20 (A) MED bilateral hip 18ys girl. (C) PO bilateral 16ys.

Fig. 21 (A), (B) Bilateral cystic necrosis & head collapsing, (C) multyple crilling and ingection of Autogenous marrow blood. (E) RAO containment of head & full coverage of Acetabulum. (F) After regeneration of F head. expecting fill up the remaining space by top osteoohyte from femoral head.
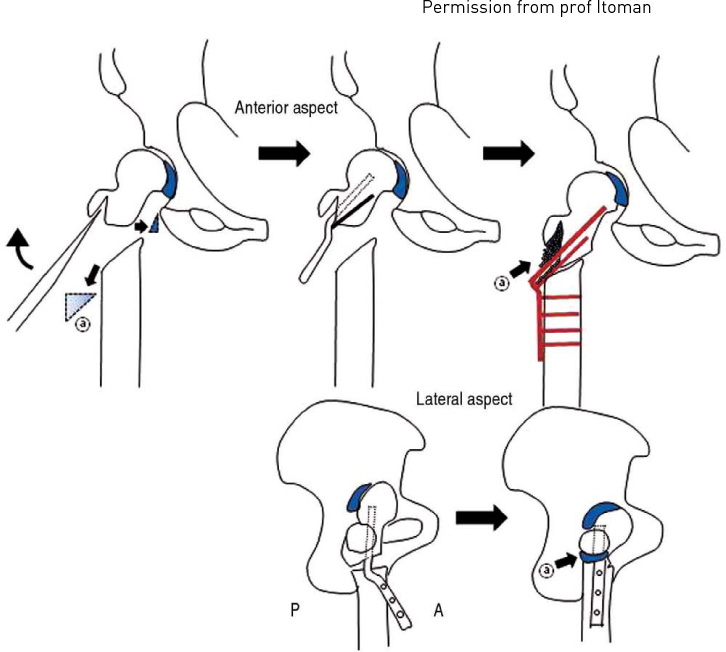
Fig. 22 The postero medial capital drop is utilized to weight bearing head surfece (paradigm shift).
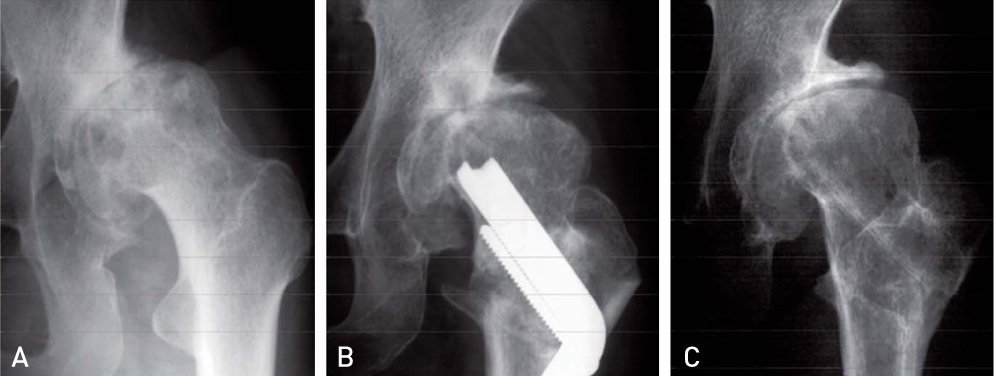
Fig. 23 Valgus flexion Osteotomy. In Tokyo Seminar/March 16, 2004; Kitasato University Hospital. (A) Pre op. 52F, (B) 1yr, (C) 18yrs.
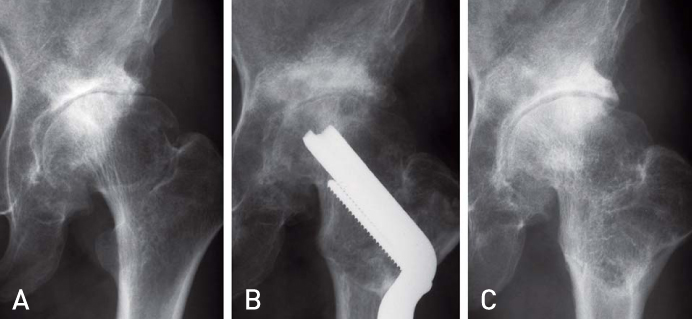
Fig. 24 (A) Preop. Hip Score-52 Roof Osteophyte, (B) 6mos. 45-o; HS=90, (C) 19yrs. HS=92.
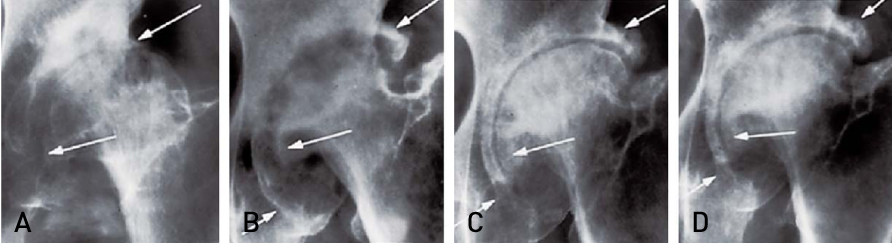
Fig. 25 The arrows are points incredible potentiality of reparative process. (A) 64 F. 1977, (B) 4yrs, (C) 11yrs, (D) 14yrs.
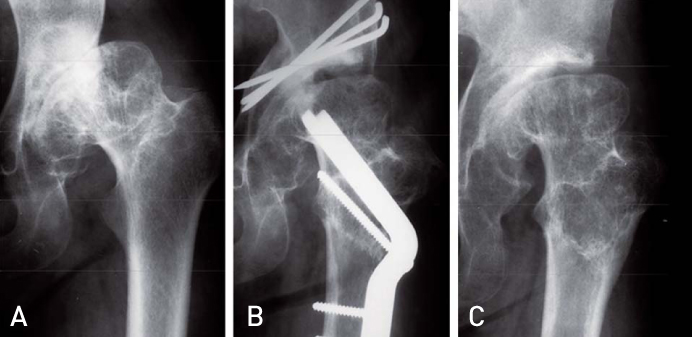
Fig. 26 48y-o. Female: AHI=55% (A) Preop, (B) 1yr, (C) 15yrs.
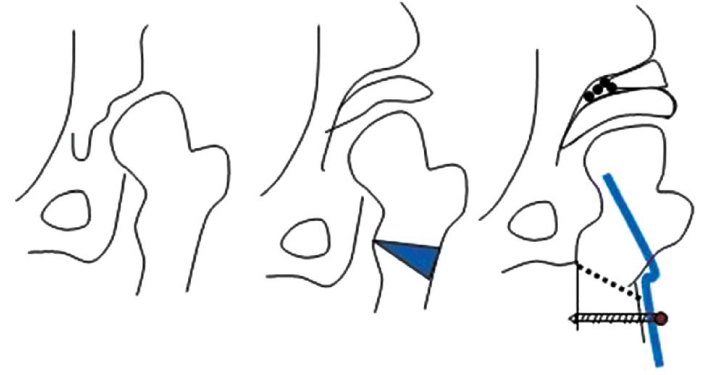
Fig. 27 In case of unsperical head, coapt the articular surpace in pararell by valgus osteotomy of proximal femur and RAO of acetabular socket.
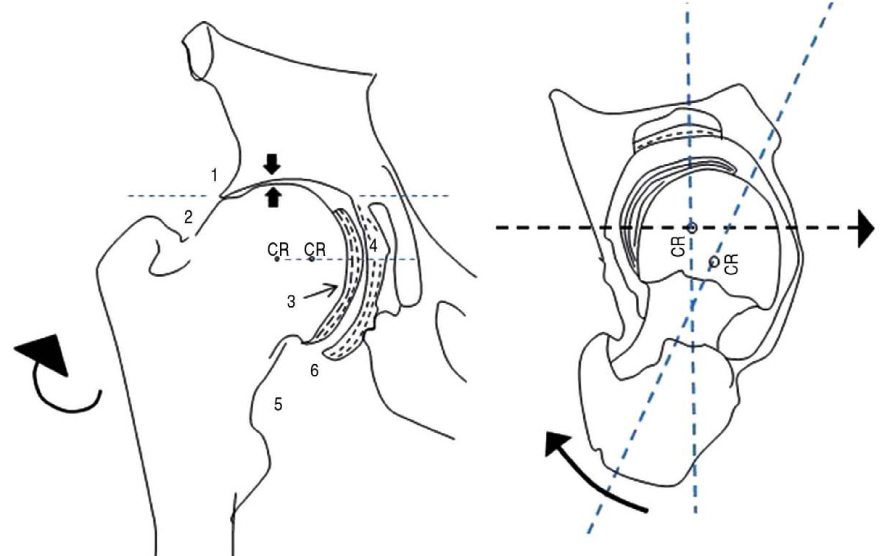
Fig. 28 1. roof, 2. superior cervical, 3. capital drop, 4. Curtain, 5. inferior cervical, 6. floor osteophyte.
Reference
-
1. Chang JS, Kwon KD, Shon HC. Bernese periacetabular osteotomy using dual approaches for hip dysplasias. J Korean Orthop Assoc. 2002. 37:226–232.
Article2. Chang JS, Park JH, Park HG, Lee SH, Kim KY. Bernese periacetabular osteotomy for hip dysplasia. J Korean Hip Soc. 1998. 10:141–148.3. Chang JS, Son HC, Pak JH, Kim KH. Acetabular osteotomy for acetabular retroversion -A case report -. J Korean Hip Soc. 2003. 15:158–161.4. Chang JS, Oh HK, Kim JW, Hong SH. Periacetabular osteotomy in hip dysplasia with deformed femoral head. J Korean Hip Soc. 2008. 43:718–727.
Article5. Eppright RH. Dial osteotomy of the acetabulum in the treatment of dysplasia of the hip. J Bone Joint Surg Am. 1975. 57-A:1172.6. Ganz R, Klaue K, Vinh TS, Mast JW. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop Relat Res. 1988. (232):26–36.
Article7. Hijikata H, Tagawa H, Toyoshima H. Rotational acetabular osteotomy with resection of capital drop. Hip Joint. 1985. 11:277–282.8. Itoman M, Yonemoto K, Sekiguchi M, Yamamoto M. Valgus-flexion osteotomy for middle-aged patients with advanced osteoarthritis of the hip: a clinical and radiological evaluation. Nihon Seikeigeka Gakkai Zasshi. 1992. 66:195–204.9. Kang CS, Shon SW, Kim SY. Rotational acetabular osteotomy for the dysplastic acetabulum. J Korean Orthop Assoc. 1986. 21:791–798.
Article10. Kang CS, Song KS, Kang CH, Lee ST, Kwon KH. Rotational acetabular osteotomy in acetabular dysplasia. J Korean Orthop Assoc. 1991. 26:1744–1755.
Article11. Kim HT, Choi SJ, Yoo CI. Bernese periacetabular osteotomy for treatment of acetabular dysplasia. J Korean Orthop Assoc. 2005. 40:942–948.
Article12. Kim HJ. Bernese periacetabular osteotomy. J Korean Hip Soc. 2001. 13:204–207.13. Kim HJ, Kim JW. Acetabular Osteotomy. J Korean Hip Soc. 2004. 16:254–260.14. Kim KH, Cho SG, Yoon TR, Song EK, Seon JK, Park GH. A new innominate osteotomy in Legg-Calve-Perthes' disease. J Korean Orthop Assoc. 2007. 42:8–15.
Article15. Min BW, Bae KC, Kang CH, Song KS, Sohn SW. Rotational acetabular osteotomy for the dysplastic hip: a follow-up for 5 to 18 years. J Korean Orthop Assoc. 2005. 40:717–722.
Article16. Naito M. A new periacetabular osteotomy for the treatment of hip dysplasia. Orthopaedic Trans. 1999.17. Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am. 1984. 66:430–436.
Article18. Atsuto Nishio. Displacement osteotomy in congenital dislocation hip. JOA. 1956. 30:483.19. Nishio Atsuto, Yoich Sugioka. Study of intertrochanteric osteotomy (Oral Presentation at WPOA Seoul, 1976). Dustrial Surg. 1971. 20:381–386.20. Park MS, Park JH, Song KH, Lee YK. Periacetabular osteotomy for treatment of acetabular dysplasia through iliofemoral approach. J Korean Hip Soc. 2006. 18:472–478.
Article21. Park YS, Moon YW, Lim SJ, Park JC, Son MS. Short-term follow-up results of periacetabular osteotomy for hip dysplasia. J Korean Hip Soc. 2009. 21:156–161.
Article22. Pemberton PA. Pericapsular osteotomy of the ilium for treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am. 1965. 47:65–86.
Article23. Salter RB. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg Br. 1961. 43-B:518–539.
Article24. Steel HH. Triple osteotomy of the innominate bone. J Bone Joint Surg Am. 1973. 55:343–350.
Article25. Hirosi Tagawa. The result of Rotational acetabular osteotomy. Ganto In Dustrial Orthopaedic. 1974. 5:409.26. Tagawa H. The treatment of coxarthrosis in adolescent and young adults. Hip Joint. 1975. 1:108–114.27. Tönnis D. Tönnis D, Legal H, Graf R, editors. Clinical and radiographic schemes for evaluating therapeutic results. Congenital dysplasia and dislocations of the hip in children and adults. 1987. 1st ed. Berlin: Springer-Verlag;165–171.
Article28. Wagner H. Weil UH, editor. Experiences with spherical acetabular osteotomy for the correction of the dysplastic acetabulum. Acetabular dysplasia: skeletal dysplasias in childhood. 1978. Berlin: Springer-Verlag;131–145.
Article29. Wagner H. Osteotomy for CDH. Proceedings in the hip society, St Louis 1976. 1976. The C.V. Mosby Co.30. Yoo MC, Cho YJ, Kim KI, Park HC, Jung CJ. Periacetabular rotational osteotomy in hip dysplasia: short term follow up result. J Korean Orthop Assoc. 2005. 40:434–441.
Article31. Yoon TR, Rowe SM, Seol JY, Cho KJ, Kim GH, Ban JS. Stress distribution according to center-edge angle in dysplastic hip and the biomechanical effect of rotational acetabular osteotomy. J Korean Orthop Assoc. 2003. 38:122–128.
Article32. Yoon TR, Cho SG, Song EK, Seon JK, Bae BH, Kong IK. Modified chiari pelvic osteotomy for dysplastic hip. J Korean Orthop Assoc. 2006. 41:960–967.
Article33. Greenwald AS. Steinberg ME, Day LJ, editors. Biomechanics of the hip. The Hip and its disorders. 1991. Philadelphia: Saunders;47–55.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rotational Acetabular Osteotomy
- Medical treatment of osteoarthritis: botanical pharmacologic aspect
- Open Access Publishing in India: Coverage, Relevance, and Future Perspectives
- Symptomatic Retinal Artery Occlusion after Angioplasty and Stenting of the Carotid Artery: Incidence and Related Risk Factors
- Current issues in osteoarthritis treatment
