Placenta percreta with a vaginal fistula after successful management by uterine transverse fundal incision and subsequent cesarean hysterectomy
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Osaka University Graduate School of Medicine, Osaka, Japan. zacky@gyne.med.osaka-u.ac.jp
- 2Department of Pathology, Osaka University Graduate School of Medicine, Osaka, Japan.
- KMID: 2051722
- DOI: http://doi.org/10.5468/ogs.2014.57.5.397
Abstract
- Placenta previa presents a highest risk to pregnancy, and placenta accreta is the most serious. Placenta accreta requires cesarean delivery and often results in massive obstetric hemorrhage and higher maternal morbidity. Challenges associated with cesarean delivery techniques may contribute to increased maternal blood loss and morbidity rates. Several recent obstetric studies reported the usefulness of transverse uterine fundal incision for managing placenta accreta. We present a case of placenta percreta that was treated by a transverse fundal incision. We successfully avoided cutting through the placenta and helped decrease maternal blood loss. After delivery, the patient underwent a cesarean hysterectomy. Postoperative day 48, she experienced watery discharge and was diagnosed with vaginal fistula. We present our case and review the literature.
MeSH Terms
Figure
-
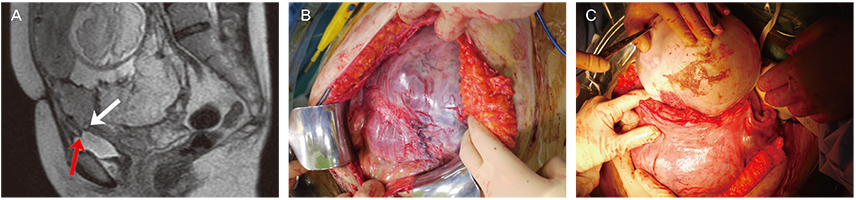
Fig. 1 (A) Magnetic resonance imaging was performed. The red arrow indicates the absence of uterine myometrium between the bladder and placenta. The white arrow indicates the placenta invades into the uterine myometrium but not deep enough to invade into the bladder muscle. (B) A laparotomy revealed multiple large blood vessels and the placenta present throughout the anterior uterine wall in the lower uterine segment. From the operative findings, we suspected placenta percreta. (C) A transverse uterine fundal incision was performed. We were careful to avoid rupturing the fetal membrane. Minimal bleeding was observed from the incision site.
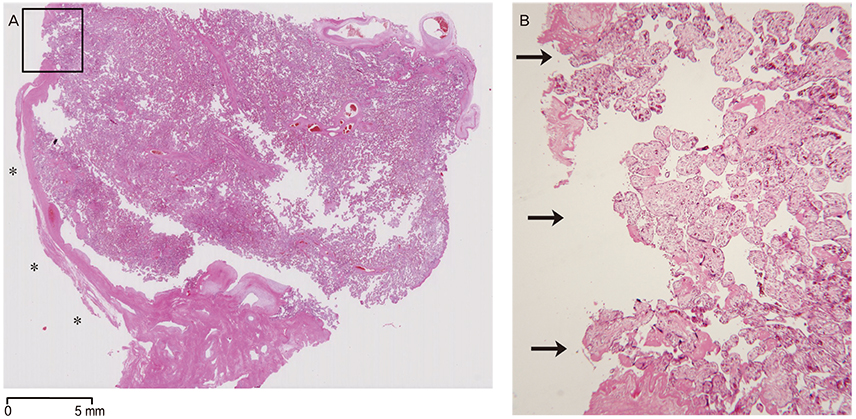
Fig. 2 (A) The loupe image of the hematoxylin and eosin-stained section of the uterus. Left side of the section (shown by the asterisks) indicates the uterine serosa. In the lesion marked by square, uterine serosa is defected by the penetration of the placenta, which is shown in higher magnitude in (B). (B) Black arrows indicate the placenta penetrating the entire myometrium to the uterine serosa (H&E, ×40).
Reference
-
1. Publications Committee, Society for Maternal-Fetal Medicine. Belfort MA. Placenta accreta. Am J Obstet Gynecol. 2010; 203:430–439.2. Matsubara S, Kuwata T, Usui R, Watanabe T, Izumi A, Ohkuchi A, et al. Important surgical measures and techniques at cesarean hysterectomy for placenta previa accreta. Acta Obstet Gynecol Scand. 2013; 92:372–377.3. Shukunami K, Hattori K, Nishijima K, Kotsuji F. Transverse fundal uterine incision in a patient with placenta increta. J Matern Fetal Neonatal Med. 2004; 16:355–356.4. Kotsuji F, Nishijima K, Kurokawa T, Yoshida Y, Sekiya T, Banzai M, et al. Transverse uterine fundal incision for placenta praevia with accreta, involving the entire anterior uterine wall: a case series. BJOG. 2013; 120:1144–1149.5. Nishida R, Yamada T, Akaishi R, Kojima T, Ishikawa S, Takeda M, et al. Usefulness of transverse fundal incision method of cesarean section for women with placentas widely covering the entire anterior uterine wall. J Obstet Gynaecol Res. 2013; 39:91–95.6. Clausen C, Lonn L, Langhoff-Roos J. Management of placenta percreta: a review of published cases. Acta Obstet Gynecol Scand. 2014; 93:138–143.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Uterine Rupture with Placenta Percreta
- A Case of Placenta Previa-Percreta Treated with Methotrexate Treatment
- A Case of Placenta Percreta Involving the Urinary Bladder
- A case of placenta previa percreta with bladder invasion
- Spontaneous uterine rupture due to placenta percreta in the second trimester of pregnancy: a case report
