Two Cases of Fractured and Embolized Implanted Central Venous Chemoports in Lung Cancer
- Affiliations
-
- 1Lung and Esophageal Cancer Clinic, Chonnam National University Hwasun Hospital, Hwasun, Korea. droij@chonnam.ac.kr
- 2Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Thoracic & Cardiovascular Surgery, Chonnam National University Medical School, Gwangju, Korea.
- 4Department of Diagnostic Radiology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2050480
- DOI: http://doi.org/10.4046/trd.2007.63.5.449
Abstract
- Totally implanted central venous access devices for chemotherapy (chemoport) are being used increasingly in lung cancer patients. Vascular catheters are associated with various complications including infection, thrombosis as well as spontaneous fractures and embolization of the catheter, which is known as 'pinch-off syndrome'. 'Pinch-off syndrome' refers to the compression of a subclavian central venous catheter between the clavicle and first rib resulting in an intermittent or permanent obstruction, which can lead to tears, transection, or embolization. We report two cases of fractured and embolized implanted subclavian venous catheters in which the fragments were removed percutaneously. A 62-year-old man presented with back pain with a duration of a few weeks. The chest radiograph revealed complete transsection and embolization of the catheter into the right atrium. In addition, a 47-year-old woman with a chemoport had a grade 3 pinch-off sign in a chest radiograph demonstrating complete transsection and embolization of the catheter into the pulmonary artery. Both cases were managed by retrieving the embolized distal fragment percutaneously and removing the proximal section of the catheter.
Keyword
MeSH Terms
Figure
-
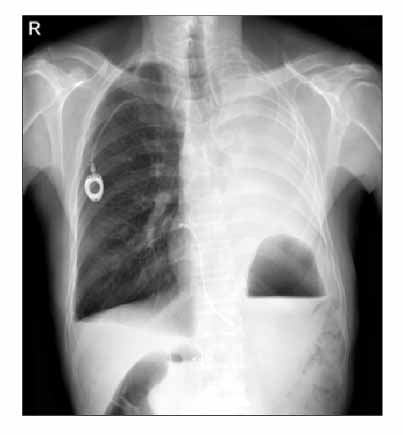
Figure 1 A chest PA illustrates the fractured catheter tip located between the right first rib and the mid-clavicle. The distal fragment is seen in the right atrium.
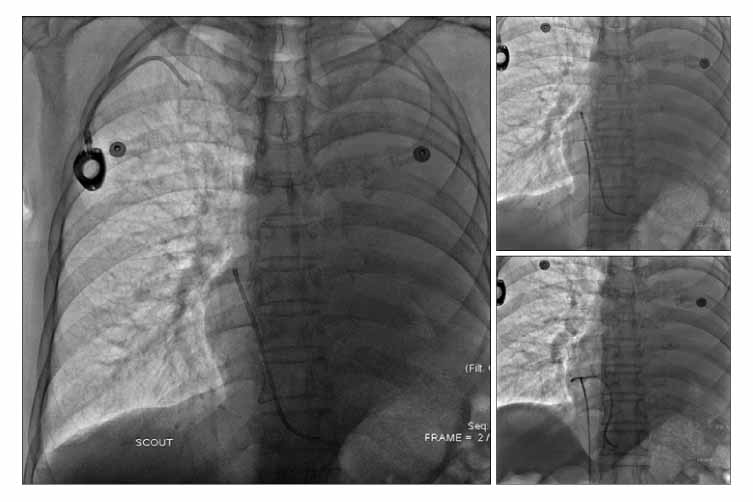
Figure 2 Inferior Vena Cavography shows a distal fractured fragment in the right atrial area (left). The right femoral vein was punctured and the fractured catheter was removed using a snare wire (right upper and lower).
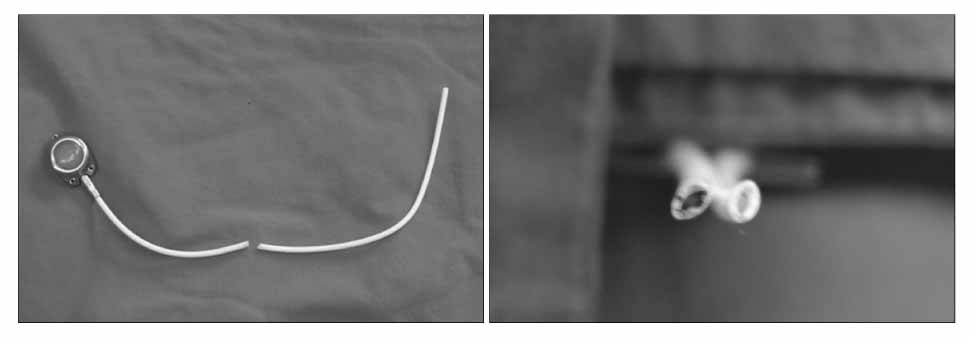
Figure 3 In a cross section, the configuration of the embolized portion of the catheter is not circular, but instead elliptical.

Figure 4 A chest PA and lateral films show the fractured chemoport catheter tip located between the left first rib and the mid-portion of the clavicle, and the distal fragment located in the main pulmonary artery.
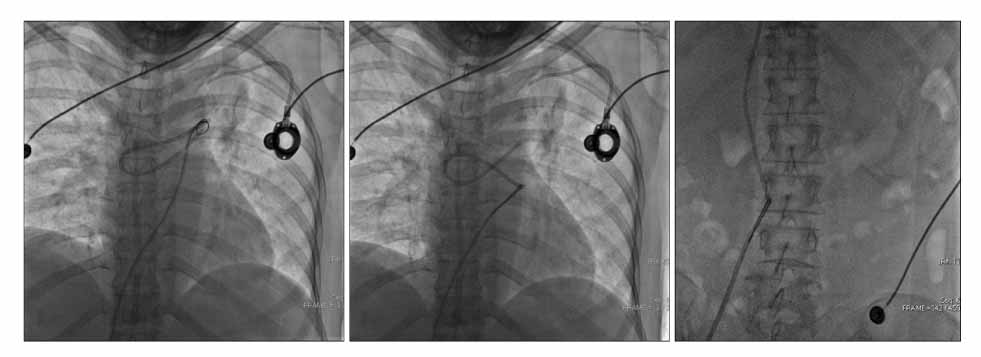
Figure 5 Removal of the distal fragment of the fractured catheter percutaneously. After the right femoral vein was punctured, the tip of the fractured chemoport was captured using a snare with a guiding catheter, and removed through the right femoral venous sheath.
Reference
-
1. Rauthe G, Altmann C. Complications in connection with venous port systems: prevention and therapy. Eur J Surg Oncol. 1998. 24:192–199.2. Yildizeli B, Lacin T, Baltacioglu F, Batirel HF, Yuksel M. Approach to fragmented central venous catheters. Vascular. 2005. 13:120–123.3. Hinke DH, Zandt-Stastny DA, Goodman LR, Quebbeman EJ, Krzywda EA, Andris DA. Pinch off syndrome: a complication of implantable subclavian venous access devices. Radiology. 1990. 177:353–356.4. Kim OK, Kim SH, Kim JB, Jeon WS, Jo SH, Lee JH, et al. Transluminal removal of a fractured and embolized indwelling central venous catheter in the pulmonary artery. Korean J Intern Med. 2006. 21:187–190.5. Coles CE, Whitear WP, Le Vay JH. Spontaneous fracture and embolization of a central venous catheter: prevention and early detection. Clin Oncol (R Coll Radiol). 1998. 10:412–414.6. McMenamin EM. Catheter fracture: a complication in venous access devices. Cancer Nurs. 1993. 16:464–467.7. Andris DA, Krzywda EA, Schulte W, Ausman R, Quebbeman EJ. Pinch-off syndrome: a rare etiology for central venous catheter occlusion. JPEN J Parenter Enteral Nutr. 1994. 18:531–533.8. Prager D, Hertzberg RW. Spontaneous intravenous catheter fracture and embolization from an implanted venous access port and analysis by scanning electron microscopy. Cancer. 1987. 60:270–273.9. Lenglinger FX, Hartl P, Kirchgatterer A, Lenglinger GM, Baldinger C. Fracture and embolization of a central venous port catheter without prior compression between the clavicle and the 1st rib. Wien Klin Wochenschr. 2001. 113:134–137.10. De Graaff JC, Bras LJ, Vos JA. Early transection of a central venous catheter in a sedated ICU patient. Br J Anaesth. 2006. 97:832–834.11. Mirza B, Vanek VW, Kupensky DT. Pinch off syndrome: case report and collective review of the literature. Am Surg. 2004. 70:635–644.12. Orsi F, Grasso RF, Arnaldi P, Bonifacio C, Biffi R, Bellomi M, et al. Ultrasound guided versus direct vein puncture in central venous port placement. J Vasc Access. 2000. 1:73–77.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Suture-Based Closure Device for Management of Inadvertent Subclavian Artery Catheterization
- A case of a fractured and impacted central venous chemoport in a patient with stomach cancer
- Transluminal Removal of a Fractured and Embolized Indwelling Central Venous Catheter in the Pulmonary Artery
- Layered Sheath-Assisted Dissection and Retrieval of Stuck Port Catheters: A Single-Center Experience
- The placement of an Implantable Chemoport via the External Jugular Vein as a Primary Route
