Anat Cell Biol.
2013 Mar;46(1):82-84. 10.5115/acb.2013.46.1.82.
A peculiar liver with surgically and radiologically important variations: a case report
- Affiliations
-
- 1Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal, Karnataka State, India. nayaksathish@gmail.com
- KMID: 2046761
- DOI: http://doi.org/10.5115/acb.2013.46.1.82
Abstract
- A peculiar liver was found in an adult male cadaver during a dissection class for undergraduate medical students. The quadrate lobe and fissure for the ligamentum teres were totally absent. Thus, the cystic notch on the inferior border was very broad and deep, and the fundus and body of the gall bladder popped out through this notch. The cystic duct terminated into the right hepatic duct at the porta hepatis instead of terminating into the common hepatic duct. Awareness of variations of the lobes and fissures may minimize a misdiagnosis of liver problems. The aim of the current study was to alert radiologists and surgeons about possible variations in the external appearance and anomalies of the lobes and fissures of the liver.
Keyword
MeSH Terms
Figure
-
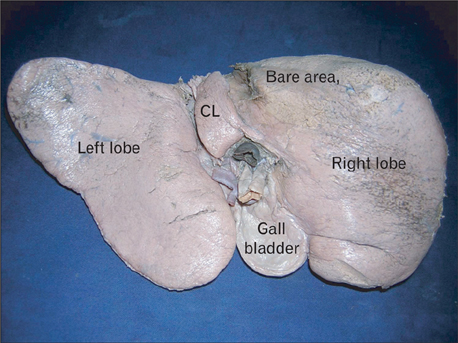
Fig. 1 Photograph of the visceral surface of the liver. Note the absence of the quadrate lobe and fissure for ligamentum teres. CL, caudate lobe.
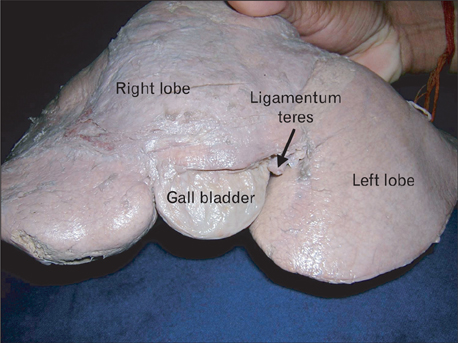
Fig. 2 Anterior view of the liver. Note the gall bladder popping out almost at the middle of the inferior border. The ligamentum teres entered the liver through the anterior surface.
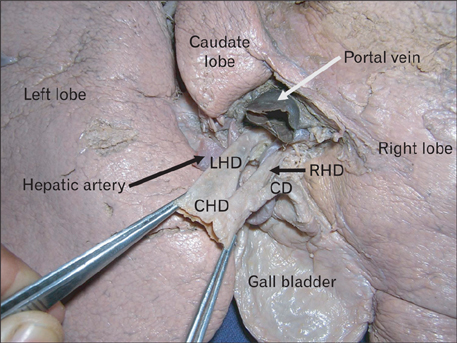
Fig. 3 Neatly displayed structures at the porta hepatis. CD, cystic duct; CHD, common hepatic duct; LHD, left hepatic duct; RHD, right hepatic duct.
Reference
-
1. Joshi SD, Joshi SS, Athavale SA. Some interesting observations on the surface features of the liver and their clinical implications. Singapore Med J. 2009. 50:715–719.2. Fitzgerald R, Hale M, Williams CR. Case report: accessory lobe of the liver mimicking lesser omental lymphadenopathy. Br J Radiol. 1993. 66:839–841.3. Llorente J, Dardik H. Symptomatic accessory lobe of the liver associated with absence of the left lobe. Arch Surg. 1971. 102:221–223.4. Gesase AP. Bifid liver presenting with anomalous quadrate and caudate lobes and a transverse gallbladder. Morphologie. 2006. 90:160–163.5. Anjamrooz SH, Azari H. Coexistence of multiple anomalies in the hepatobiliary system. Anat Cell Biol. 2012. 45:62–65.6. Othman FB, Latiff AA, Suhaimi FH, Das S. Accessory sulci of the liver: an anatomical study with clinical implications. Saudi Med J. 2008. 29:1247–1249.7. Ogawa T, Ohwada S, Ikeya T, Shiozaki H, Aiba S, Morishita Y. Left-sided gallbladder with anomalies of the intrahepatic portal vein and anomalous junction of the pancreaticobiliary ductal system: a case report. Hepatogastroenterology. 1995. 42:645–649.8. Si-Youn R, Poong-Man J. Left-sided gallbladder with right-sided ligamentum teres hepatis: rare associated anomaly of exomphalos. J Pediatr Surg. 2008. 43:1390–1395.9. Pamidi N, Nayak S, Vollala VR. Cystogastrocolic fold and associated atrophy of the gallbladder. Singapore Med J. 2008. 49:e250–e251.10. Nayak SB. Abnormal peritoneal fold connecting the greater omentum with the liver, gallbladder, right kidney and lesser omentum. Bratisl Lek Listy. 2009. 110:736–737.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Vascular Variations in Posterior Abdominal Region: A Case Report
- Vascular variations of liver and gallbladder: a case report
- Two-stage liver transplantation in a surgically complicated liver failure patient after hepatic tumor resection: A case report
- Portal vein fenestration: a case report of an unusual portal vein developmental anomaly
- Well-differentiated osteosarcoma of the rib.
