J Clin Neurol.
2009 Sep;5(3):146-148. 10.3988/jcn.2009.5.3.146.
Secondary Amyloidosis Associated with Multiple Sclerosis
- Affiliations
-
- 1Department of Neurology, Hanyang University College of Medicine, Guri, Korea. ksh213@hanyang.ac.kr
- 2Department of Internal Medicine, Hanyang University College of Medicine, Guri, Korea.
- 3Department of Pathology, Hanyang University College of Medicine, Guri, Korea.
- KMID: 2045421
- DOI: http://doi.org/10.3988/jcn.2009.5.3.146
Abstract
- BACKGROUND
Multiple sclerosis (MS) is a demyelinating disease of the central nervous system. Secondary amyloidosis can occur as a complication of chronic systemic inflammatory and infectious diseases. Until now there has been no report of secondary amyloidosis associated with MS. We report herein a case of renal biopsy-proven secondary amyloidosis in a patient with MS. CASE REPORT: A 41-year-old woman with MS was hospitalized due to aggravated quadriparesis and edema in both lower extremities. Laboratory findings showed nephrotic-range proteinuria and hypoalbuminemia. A percutaneous renal biopsy procedure was performed, the results of which revealed secondary amyloid-A-type amyloidosis associated with MS. CONCLUSIONS: This is the first report of secondary amyloidosis associated with MS.
MeSH Terms
Figure
-
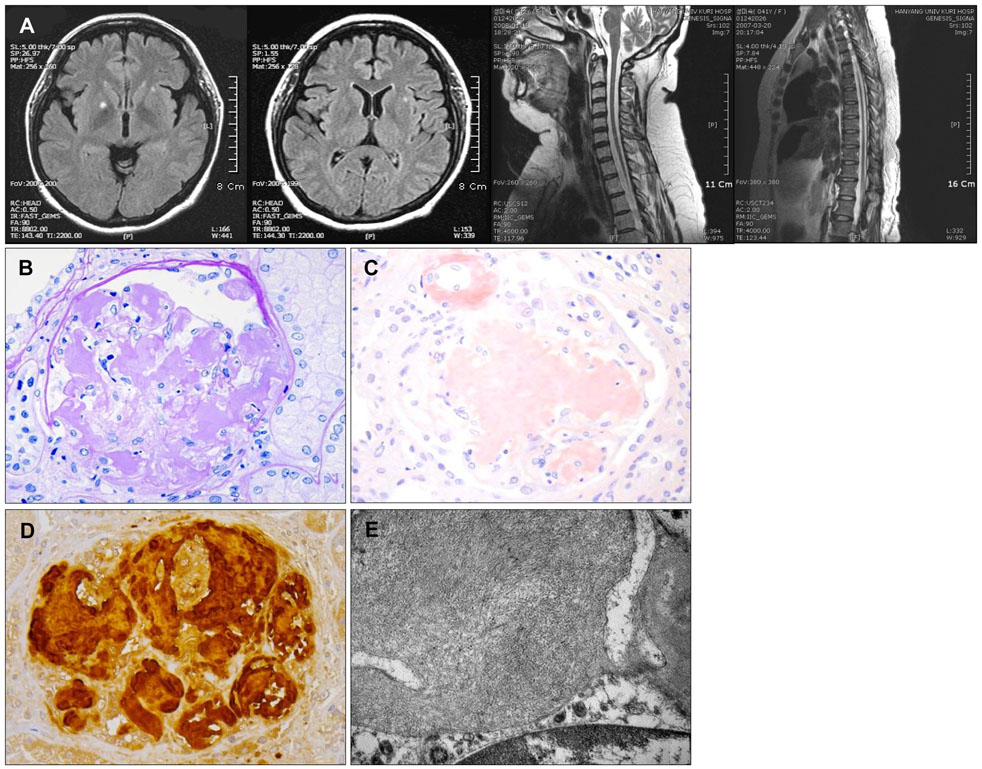
Fig. 1 MRI and microscopic findings. A: Fluid-attenuated inversion recovery sequence on MRI showing three plaques in the brain, and T2-weighted MRI showing severe atrophy of the cervical and thoracic cord. B: On light microscopy, the glomerulus exhibits extensive effacement of the glomerular architecture by large, irregularly shaped, amorphous, weakly periodic acid-Schiff (PAS)-positive, amyloid deposits (PAS ×400). C: Strongly Congoredpositive materials can be seen in the glomeruli and arterioles (Congoed, ×400). D: Amyloid deposits are positive on immunohistochemical staining for AA. E: Note the large nodular mesangial deposition of nonbranching, thin fibrils, ranging from 8.33 to 13.1 nm in thickness (electron micrograph, ×25,000).
Reference
-
1. Compston A, Coles A. Multiple sclerosis. Lancet. 2002. 359:1221–1231.
Article2. Uda H, Yokota A, Kobayashi K, Miyake T, Fushimi H, Maeda A, et al. Two distinct clinical courses of renal involvement in rheumatoid patients with AA amyloidosis. J Rheumatol. 2006. 33:1482–1487.3. Schroöder R, Nennesmo I, Linke RP. Amyloid in a multiple sclerosis lesion in clearly of Alambda type. Acta Neuropathol. 2000. 100:709–711.4. Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med. 1997. 337:898–909.
Article5. Lachmann HJ, Goodman HJ, Gilbertson JA, Gallimore JR, Sabin CA, Gillmore JD, et al. Natural history and outcome in systemic AA amyloidosis. N Engl J Med. 2007. 356:2361–2371.
Article6. Livneh A, Zemer D, Langevitz P, Laor A, Sohar E, Pras M. Colchicine treatment of AA amyloidosis of familial Mediterranean fever. An analysis of factor affecting outcome. Arthritis Rheum. 1994. 37:1804–1811.7. Tuglular S, Yalcinkaya F, Paydas S, Oner A, Utas C, Bozfakioglu S, et al. A retrospective analysis for aetiology and clinical findings of 287 secondary amyloidosis cases in Turkey. Nephrol Dial Transplant. 2002. 17:2003–2005.
Article8. Ristori G, Laurenti F, Stacchini P, Gasperini C, Buttinelli C, Pozzilli C, et al. Serum amyloid A protein is elevated in relapsing-remitting multiple sclerosis. J Neuroimmunol. 1998. 88:9–12.
Article9. Schwimmer JA, Joseph RE, Appel GB. Wilcox CS, Brady HR, editors. Amyloid, fibrillary, and the glomerular deposition disease in therapy. Nephrology and Hypertension. 2003. Philadelphia: Saunders;253–261.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic Findings of Secondary Systemic Amyloidosis Associated with Tuberculosis: A Case Report
- A Case of Biphasic Amyloidosis in Systemic Sclerosis
- A Case of Macroglossia due to Amyloidosis Associated with Multiple Myeloma
- AL amyloidosis: advances in diagnosis and management
- Multiple Skeletal Involvement of Multiple Myeloma Associated Amyloidosis Presented with Pathologic Fracture
