Biliary Obstruction Caused by Intra-Biliary Tumor Growth from Recurred Hepatocellular Carcinoma after Radiofrequency Ablation: Case Report
- Affiliations
-
- 1Department of Radiology, Yeungnam University College of Medicine, Daegu, Korea. sungho1999@ynu.ac.kr
- KMID: 2041941
- DOI: http://doi.org/10.3348/jksr.2014.70.4.295
Abstract
- A 59-year-old man with a known central hepatocellular carcinoma (HCC) underwent a trans-arterial-chemo-embolization (TACE) and a post-TACE percutaneous radiofrequency ablation (PRFA). Two months after the PRFA, the patient presented jaundice and an abdominal computed tomography was obtained. An arterial enhancing mass adjacent to the ablated necrotic lesion with a continuously coexisting mass inside the right hepatic duct, suggestive of a HCC recurrence with a direct extension to the biliary tract was found. Finally a biliary tumor obstruction has been developed and a percutaneous transhepatic biliary drainage was performed. This case of biliary obstruction caused by directly invaded recurred HCC after PRFA will be reported because of its rare occurence.
MeSH Terms
Figure
-

Fig. 1 Transverse CT scans in 60-year-old man with prior trans-arterial embolization and radiofrequency ablation due to central located hepatocellular carcinoma. A. Arterial phase scan shows lipiodol uptake lesions is located in the ablation necrosis which is central portion of the liver. B. The same CT scan in hepatic hilum level demonstrates early enhancing mass (black arrow) at the hepatic hilum is abutting upon the right hepatic duct (white arrow). The mass is located just below the necrotic thermal lesion. C. On portal phase scan, the mass is extending into the common hepatic duct (black arrow) and portal vein thrombus (gray arrow) is also noted.
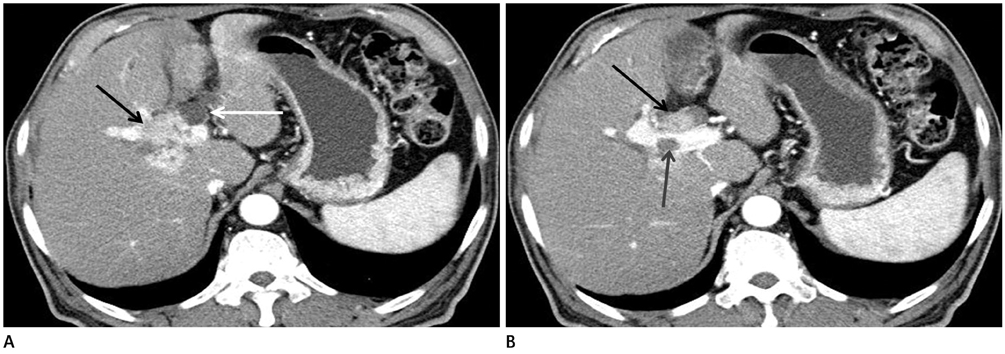
Fig. 2 Two months after follow-up transverse scans follow of the same patient. A. Arterial phase scan reveals early enhancing mass (black arrow) at hepatic hilum was increased in size with dilated adjacent right hepatic duct (white arrow). B. On the same CT scan, the intra-biliary growing of the mass (black arrow) and portal vein thrombosis (gray arrow) are more prominent with biliary dilatation.
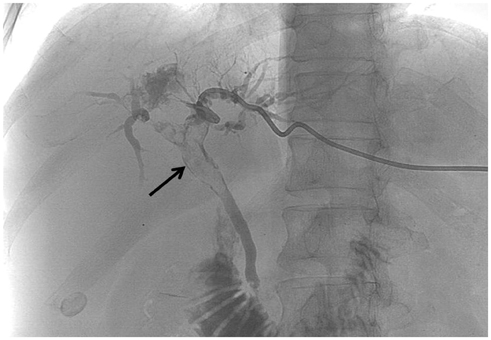
Fig. 3 Percutaneous transhepatic cholangiography which was obtained 20 days after follow-up CT demonstrated more extended mass represented as filling defect (black arrow) in the both intra-hepatic duct, common hepatic duct, and common bile duct without dilatation of biliary ducts.
Reference
-
1. Qin LX, Tang ZY. Hepatocellular carcinoma with obstructive jaundice: diagnosis, treatment and prognosis. World J Gastroenterol. 2003; 9:385–391.2. Lee JW, Han JK, Kim TK, Choi BI, Park SH, Ko YH, et al. Obstructive jaundice in hepatocellular carcinoma: response after percutaneous transhepatic biliary drainage and prognostic factors. Cardiovasc Intervent Radiol. 2002; 25:176–179.3. Long XY, Li YX, Wu W, Li L, Cao J. Diagnosis of bile duct hepatocellular carcinoma thrombus without obvious intrahepatic mass. World J Gastroenterol. 2010; 16:4998–5004.4. Abe T, Kajiyama K, Harimoto N, Gion T, Shirabe K, Nagaie T. Intrahepatic bile duct recurrence of hepatocellular carcinoma without a detectable liver tumor. Int J Surg Case Rep. 2012; 3:275–278.5. Qin LX, Ma ZC, Wu ZQ, Fan J, Zhou XD, Sun HC, et al. Diagnosis and surgical treatments of hepatocellular carcinoma with tumor thrombosis in bile duct: experience of 34 patients. World J Gastroenterol. 2004; 10:1397–1401.6. Chen MF, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC. Obstructive jaundice secondary to ruptured hepatocellular carcinoma into the common bile duct. Surgical experiences of 20 cases. Cancer. 1994; 73:1335–1134.7. Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics. 2003; 23:123–134.8. Sasahira N, Tada M, Yoshida H, Tateishi R, Shiina S, Hirano K, et al. Extrahepatic biliary obstruction after percutaneous tumour ablation for hepatocellular carcinoma: aetiology and successful treatment with endoscopic papillary balloon dilatation. Gut. 2005; 54:698–702.9. Kubota Y, Seki T, Kunieda K, Nakahashi Y, Tani K, Nakatani S, et al. Biliary endoprosthesis in bile duct obstruction secondary to hepatocellular carcinoma. Abdom Imaging. 1993; 18:70–75.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biliary Fistula Developed after Radiofrequency Ablation Therapy for Hepatocellular Carcinoma
- Biliary-duodenal Fistula Following Radiofrequency Ablation Therapy for Hepatocellular Carcinoma
- Radiofrequency Ablation of Hepatic Cysts: Case Report
- Role of radiofrequency ablation in advanced malignant hilar biliary obstruction
- Management of Obstructive Jaundice Caused by Hepatocellular Carcinoma
