Interventional and Surgical Treatment of a Hemothorax Caused by a Ruptured Vertebral Artery in a Patient with Neurofibromatosis Type I
- Affiliations
-
- 1Department of Radiology, Chosun University College of Medicine, Gwangju, Korea. dhk0827@chosun.ac.kr
- 2Department of Cardiovascular Surgery, Chosun University College of Medicine, Gwangju, Korea.
- KMID: 2041933
- DOI: http://doi.org/10.3348/jksr.2014.70.4.247
Abstract
- We report a case of a massive hemothorax arising from a ruptured vertebral artery aneurysm in a patient with neurofibromatosis type 1 suffering from sudden onset of dyspnea. The vertebral artery aneurysm was treated with endovascular coil embolization. Then, an open thoracotomy was performed to evacuate the hematoma.
MeSH Terms
Figure
-
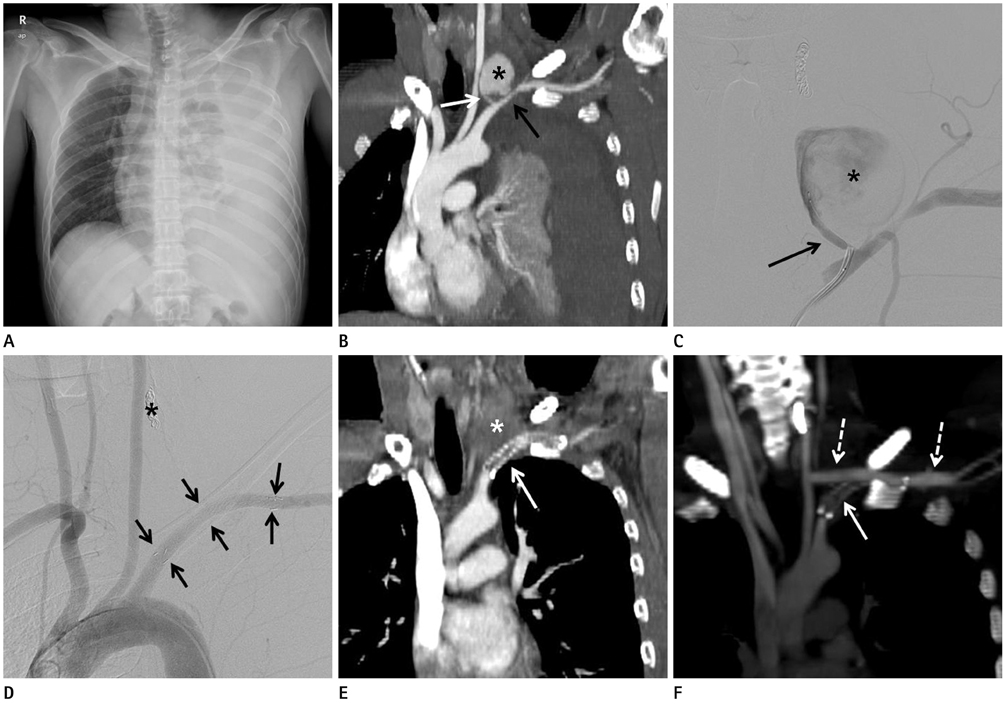
Fig. 1 A 34-year-old man with neurofibromatosis. A. Chest radiography reveals a large degree of left pleural effusion with passive atelectasis. The trachea has also shifted to the right side. B. Thoracic CT angiography reveals a pseudoaneurysm (asterisk) 3.8 cm in size in the left proximal vertebral artery (white arrow). The left subclavian artery (black arrow) is compressed by an aneurysm with a hematoma. C. Vertebral angiography after embolization with a microcoil was performed to treat a pseudoaneurysm (asterisk) 3.8 cm in size originating from the left proximal vertebral artery (black arrow) and an 80% narrowing of the left mid-subclavian artery. D. Thoracic aortography after coil embolization (asterisk) and stent deployment (arrows) shows patency of left subclavian artery and occlusion of distal portion of left vertebral artery. E. On thoracic CT performed 13 days after embolization and surgery, an in-stent occlusion within the left subclavian artery (arrow) attached to a perivertebral hematoma (asterisk) is detected. F. An oblique coronal CT scan with maximal intensity projection shows good patency within the left common carotid artery to the left subclavian artery bypass graft (dotted arrows) and an occluded stent in the left subclavian artery (arrow).
Reference
-
1. Hirsch NP, Murphy A, Radcliffe JJ. Neurofibromatosis: clinical presentations and anaesthetic implications. Br J Anaesth. 2001; 86:555–564.2. Niimi M, Ikeda Y, Kan S, Takami H, Furui S, Takeshita K. Re: spontaneous rupture of an intercostal artery due to neurofibromatosis type I disease treated by percutaneous embolization. Cardiovasc Intervent Radiol. 2002; 25:160–161.3. Kim SJ, Kim CW, Kim S, Lee TH, Kim KI, Moon TY, et al. Endovascular treatment of a ruptured internal thoracic artery pseudoaneurysm presenting as a massive hemothorax in a patient with type I neurofibromatosis. Cardiovasc Intervent Radiol. 2005; 28:818–821.4. Hongsakul K, Rookkapan S, Tanutit P, Pakdeejit S, Songjamrat A, Sungsiri J. Spontaneous massive hemothorax in a patient with neurofibromatosis type 1 with successful transarterial embolization. Korean J Radiol. 2013; 14:86–90.5. Hall RJ, Miller GA, Kerr IH. Ruptured bronchial artery aneurysm mimicking aortic dissection. Br Heart J. 1977; 39:909–910.6. Miyazaki T, Ohta F, Daisu M, Hoshii Y. Extracranial vertebral artery aneurysm ruptured into the thoracic cavity with neurofibromatosis type 1: case report. Neurosurgery. 2004; 54:1517–1520.7. Salyer WR, Salyer DC. The vascular lesions of neurofibromatosis. Angiology. 1974; 25:510–519.8. Lehrnbecher T, Gassel AM, Rauh V, Kirchner T, Huppertz HI. Neurofibromatosis presenting as a severe systemic vasculopathy. Eur J Pediatr. 1994; 153:107–109.9. Chang WC, Hsu HH, Chang H, Chen CY. Spontaneous hemothorax caused by a ruptured intercostal artery aneurysm in von Recklinghausen's neurofibromatosis. J Formos Med Assoc. 2005; 104:286–289.10. Dominguez J, Sancho C, Escalante E, Morera JR, Moya JA, Bernat R. Percutaneous treatment of a ruptured intercostal aneurysm presenting as massive hemothorax in a patient with type I neurofibromatosis. J Thorac Cardiovasc Surg. 2002; 124:1230–1232.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Hemothorax Caused by Rupture of an Intercostal Artery Aneurysm in Neurofibromatosis Type I I : A Case Report
- Spontaneous Extracranial Vertebral Artery Dissection in a Neurofibromatosis 1 Patient with Bilateral Intrathoracic Spinal Meningoceles around the Scoliosis: Report of an Autopsy Case
- Spontaneous Massive Hemothorax in a Patient with Neurofibromatosis Type 1 with Successful Transarterial Embolization
- Spontaneous Hemothorax in a Patient with Type I Neurofibromatosis
- Endovascular Treatment of a Ruptured Internal Mammary Artery Pseudoaneurysm Presenting as Massive Hemothorax in a Patient with Type I Neurofibromatosis
