A Case of Coronary Artery Dissection After Aortic Replacement in Acute Type A Aortic Dissection
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea. hspark@knu.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Kyungpook National University Hospital, Daegu, Korea.
- KMID: 2028924
- DOI: http://doi.org/10.4070/kcj.2009.39.10.428
Abstract
- A 59-year-old woman was transferred to our institution with a diagnosis of acute type A aortic dissection. During aortic replacement surgery, the dissection had not extended to the orifice of the left coronary artery. However, ST segment elevation was observed on an electrocardiogram monitor immediately postoperatively. An emergent coronary angiogram showed almost complete collapse of the lumen of the left coronary artery due to pulsatile compression of the false lumen, which was caused by extension of the aortic dissection. Percutaneous coronary intervention (PCI) was performed with placement of stents in the left anterior descending artery (LAD) and left circumflex artery. Coronary angiography and intravascular ultrasound performed 45-days after PCI showed significant instent restenosis (ISR) at the proximal portion of the LAD and residual coronary artery dissection of the diagonal branch. Repeat balloon angioplasty was performed at the site of the ISR. A follow-up coronary angiogram 8-months after the PCI showed no evidence of ISR.
Keyword
MeSH Terms
Figure
-
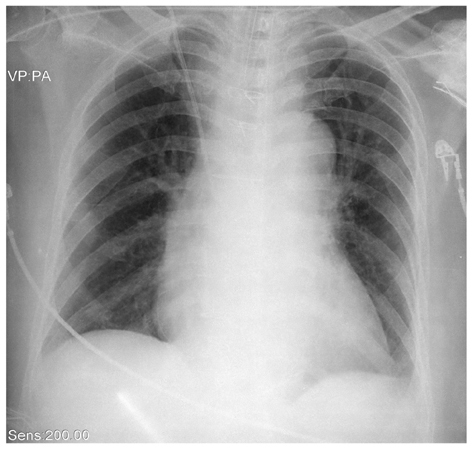
Fig. 1 Chest X-ray showing mediastinal widening.
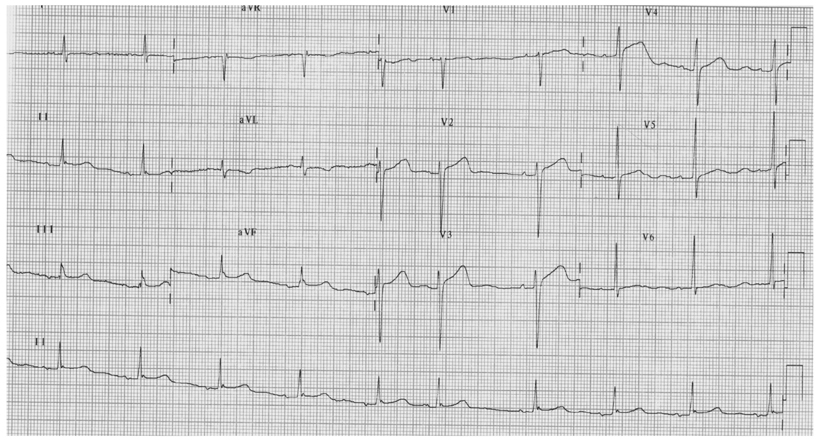
Fig. 2 Initial electrocardiogram showed normal sinus rhythm with a premature atrial complex. There were no significant ST-T changes.

Fig. 3 Emergent computed tomogram of the chest showing an acute Stanford type A aortic dissection (A). The left coronary artery had good patency and no dissection (B).

Fig. 4 Electrocardiography demonstrated ST segment elevation in leads II, III, and aVF, and in the precordial leads immediately postoperatively.
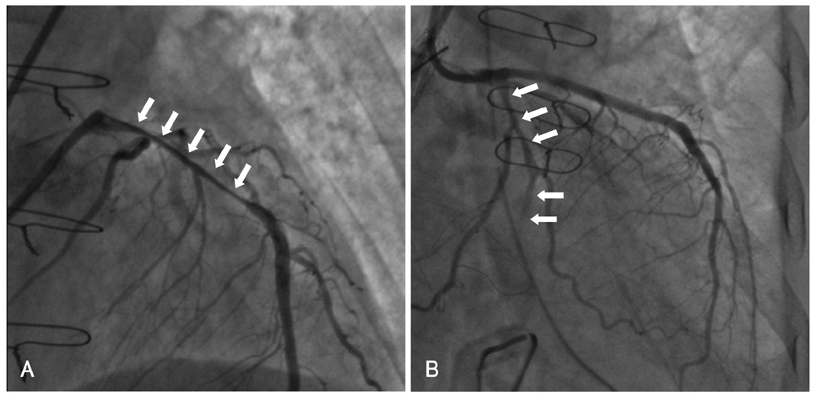
Fig. 5 Postoperative emergent coronary angiogram showing almost complete collapse of the lumen of the left anterior descending artery (A). After forceful contrast injection into the left anterior descending artery, the lumen of the collapsed left anterior descending artery which had been reopened, subsequently recollapsed (arrows). The dissection encircled the affected coronary ostium and the observed malperfusion was produced by direct coronary blood flow obstruction. Similar findings were obtained in the left circumflex artery (arrows) (B).

Fig. 6 Follow-up coronary angiogram performed 45-days after percutaneous coronary intervention showing significant in-stent restenosis at the proximal portion of the left anterior descending artery in the anteroposterior caudal (arrow) (A) and in the left anterior oblique caudal views (arrow) (B).

Fig. 7 The intravascular ultrasound study showed significant in-stent restenosis in the proximal portion of the left anterior descending artery and remaining coronary artery dissection in the diagonal branch of the left anterior descending artery (*). There was no significant instent restenosis or remaining dissection of the left circumflex artery.

Fig. 8 Follow-up coronary angiogram performed 8 months after percutaneous coronary intervention showing no significant in-stent restenosis.
Reference
-
1. Nah DY, Park KU, Kim SH. Acute proximal aortic dissection associated with ST segment elevation on electrocardiography. Korean Circ J. 2004. 34:795–798.2. Kawahito K, Adachi H, Murata S, Yamaguchi A, Ino T. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management. Ann Thorac Surg. 2003. 76:1471–1476.3. Neri E, Toscano T, Papalia U, et al. Proximal aortic dissection with coronary malperfusion: presentation, management, and outcome. J Thorac Cardiovasc Surg. 2001. 121:552–560.4. Kwon YS, Lee HS, Shin JK, et al. A case of left main coronary stenting for acute myocardial infarction complicated by ascending aortic dissection. Korean Circ J. 2004. 34:1210–1215.5. Horszczaruk GJ, Roik MF, Kochman J, et al. Aortic dissection involving ostium of right coronary artery as the reason of myocardial infarction. Eur Heart J. 2006. 27:518.6. Weber M, Kerber S, Rahmel A, Breithardt G, Diallo S, Bocker W. Acute thoracic aortic dissection with occlusion of the left coronary artery. Herz. 1997. 22:104–110.7. Geirsson A, Szeto WY, Pochettino A, et al. Significance of malperfusion syndromes prior to contemporary surgical repair for acute type A dissection: outcomes and need for additional revascularizations. Eur J Cardiothorac Surg. 2007. 32:255–262.8. Hirst AE Jr, Jones VJ Jr, Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine. 1958. 37:217–279.9. Kawada T, Okada Y, Aiba M, et al. Changing predictors of postoperative mortality in acute type A aortic dissection: is only coronary artery compromise significant? Jpn J Thorac Cardiovasc Surg. 2001. 49:347–354.10. DeSanctis RW, Doroghagi RM, Austen WG, Buckley MJ. Aortic dissection. N Engl J Med. 1987. 317:1060–1067.11. Na SH, Youn TJ, Cho YS, et al. Acute myocardial infarction caused by extension of a proximal aortic dissection flap into the right coronary artery: an intracoronary ultrasound image. Circulation. 2006. 113:e669–e671.12. Ohuchi H, Kyo S, Matsumura M, et al. Global myocardial ischemia as a complication of an acute type A aortic dissection: rapid diagnosis of a case by transesophageal echocardiography. Jpn Circ J. 2000. 64:533–536.13. Penn MS, Smedira N, Lytle B, Brener SJ. Does coronary angiography before emergency aortic surgery affect in-hospital mortality? J Am Coll Cardiol. 2000. 35:889–894.14. Funatsu T, Fukuda H, Takeuchi M, Masai M, Kawano S, Abe K. Progression of left coronary artery dissection during and after aortic replacement in acute type A aortic dissection: a case report. Ann Thorac Cardiovasc Surg. 2007. 13:209–212.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Total Aortic Arch Replacement with Root Plasty with Right Coronary Artery Bypass and Distal Open Stent-graft Insertion in Acute Type I Aortic Dissection
- Endovascular Treatment of Aortic Dissection due to Suture Line Dehiscence after Aortic Graft Replacement for Type A Aortic Dissection: A Report of Two Cases
- Total Arch Replacement with Stented Elephant Trunk in DeBakey Type I Acute Aortic Dissection
- Comparison of the Mid-term Changes at the Remnant Distal Aorta after Aortic Arch Replacement or Ascending Aortic Replacement for Treating Type A Aortic Dissection
- Total Arch Replacement for Chronic Aortic Aneurysmal Dissection Patient with Aberrant Subclavian Artery
