Korean Circ J.
2009 Oct;39(10):418-422. 10.4070/kcj.2009.39.10.418.
Prevalence and Positive Predictive Value of Poor R-Wave Progression and Impact of the Cardiothoracic Ratio
- Affiliations
-
- 1Department of Internal Medicine, University of Ulsan College of Medicine, Seoul, Korea. youho@amc.seoul.kr
- 2Center for Clinical Service, National Cancer Center, Goyang, Korea.
- KMID: 2028922
- DOI: http://doi.org/10.4070/kcj.2009.39.10.418
Abstract
- BACKGROUND AND OBJECTIVES
Poor R-wave progression (PRWP) is a common electrocardiographic diagnosis. However, the diagnostic usefulness of PRWP for coronary artery disease (CAD) and the plausible explanation for subjects with normal heart function are unclear. SUBJECTS AND METHODS: We included 20,739 subjects who had routine medical examinations and applied the commonly used criteria (R-waves in V3 or V4 < or =2 mm) and the Marquette criteria in the current study. Subjects with PRWP by the Marquette criteria, but with no evidence of specific causes, were identified. Healthy age- and gender-matched controls were selected randomly for comparing cardiothoracic ratios. RESULTS: The commonly used criteria in practice were met by 372 of the 20,739 subjects (1.8%). The Marquette criteria were met by 96 subjects (0.5%), and 82 of who agreed to medical evaluation. Five subjects had known CAD and only one subject was shown to have a silent myocardial infarction by additional testing. Therefore, the positive predictive value of PRWP for CAD was 7.3% (6/82) based on the Marquette criteria. As compared with the control group, the subjects with PRWP had a significantly low cardiothoracic ratio (0.425 vs. 0.445, p<0.05), especially among the male group (0.454 vs. 0.407, p=0.02). CONCLUSION: The positive predictive value of PRWP for CAD in the general population is so low that additional tests for diagnosis may be unreasonable. In addition, a low cardiothoracic ratio could be a plausible explanation of PRWP in subjects without any identifiable cause.
MeSH Terms
Figure
-
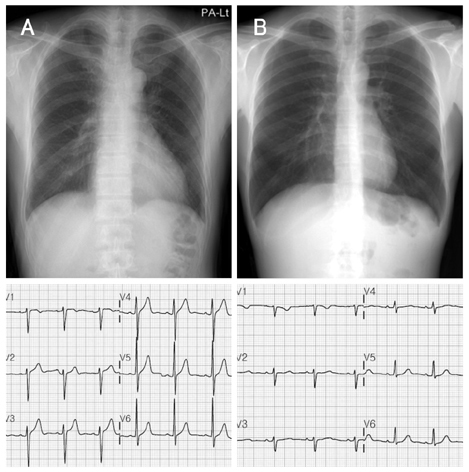
Fig. 1 Chest radiographs and electrocardiogram in a normal control subject (A) showing a normal cardiothoracic ratio, and in a subject with PRWP (B) showing a low cardiothoracic ratio. PRWP: poor R-wave progression.
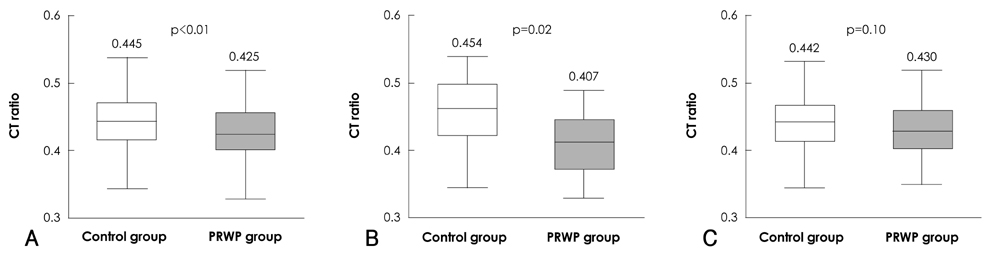
Fig. 2 Box plots comparing cardiothoracic ratios in the control and PRWP groups. The cardiothoracic ratio is significantly associated with the presence of PRWP in all (A) and male subjects (B) although it is not in female subjects (C). The central boxes include the middle 50 percentile of the data and horizontal lines show the middle of 80 percentile of data. CT ratios: cardiothoracic ratios, PRWP: poor R-wave progression.
Reference
-
1. Physician's Guide to Marquette Electronics Resting ECG Analysis. 1991. Milwaukee, Wis: Marquette Electronics Inc.2. DePace NL, Colby J, Hakki AH, Manno B, Horowitz LN, Iskandrian AS. Poor R wave progression in the precordial leads: clinical implications for the diagnosis of myocardial infarction. J Am Coll Cardiol. 1983. 2:1073–1079.3. Wagner A, Mahrholdt H, Holly TA, et al. Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet. 2003. 361:374–379.4. Zema MJ, Collins M, Alonso DR, Kligfield P. Electrocardiographic poor R-wave progression: correlation with postmortem findings. Chest. 1981. 79:195–200.5. Joo IJ, Hur DY, Kim ES, et al. Differential diagnosis in cases showeing poor R-wave progression on EKG by ventorcardiography. Korean Circ J. 1986. 16:349–356.6. Won KH, Chang MY, Oh KS, Kim YC, Lee HC. Clinical observation on poor R-wave progression. Korean Circ J. 1983. 13:195–201.7. Wagner GS. Marriott's Practical Electrocardiography. 2001. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins.8. Zema MJ, Kligfield P. Electrocardiographic poor R wave progression: I. correlation with the Frank vectorcardiogram. J Electrocardiol. 1979. 12:3–10.9. Zaman MJ, Sanders J, Crook AM, et al. Cardiothoracic ratio within the "normal" range independently predicts mortality in patients undergoing coronary angiography. Heart. 2007. 93:491–494.10. Feldman T, Borow KM, Neumann A, Lang RM, Childers RW. Relation of electrocardiographic R-wave amplitude to changes in left ventricular chamber size and position in normal subjects. Am J Cardiol. 1985. 55:1168–1174.11. Sugita S, Takada K, Takada H, Nagashima M, Hayano J. The relationship between R amplitude in lead V5 (RV5) and left ventricular mass in the groups of adolescent subjects classified by body composition. Jpn Circ J. 1998. 62:893–899.12. Gami AS, Holly TA, Rosenthal JE. Electrocardiographic poor R-wave progression: analysis of multiple criteria reveals little usefulness. Am Heart J. 2004. 148:80–85.13. Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N. Unrecognized myocardial infarction: epidemiology, clinical characteristics, and the prognostic role of angina pectoris. Ann Intern Med. 1995. 122:96–102.14. Kannel WB, Cupples LA, Gagnon DR. Incidence, precursors and prognosis of unrecognized myocardial infarction. Adv Cardiol. 1990. 37:202–214.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A study on computed tomography cardiothoracic ratio in predicting left ventricular systolic dysfunction
- Clinical Observation on Poor R-Wave Progression
- The Different Inspiratory Pressure Waves in Variuos I:E Ratio : Comparison of the Oxygenation and Ventilation in F1O2 1.0
- A CT Criteria of Cardiomegaly
- Impact of Glycemic Control and Metformin Use on the Recurrence and Progression of Non-Muscle Invasive Bladder Cancer in Patients with Diabetes Mellitus
