Extraneural Metastasis of Glioblastoma Multiforme Presenting as an Unusual Neck Mass
- Affiliations
-
- 1Department of Neurosurgery & Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. mdcwh@naver.com
- KMID: 2018188
- DOI: http://doi.org/10.3340/jkns.2012.51.3.147
Abstract
- Glioblastoma multiforme (GBM) is the most aggressive intracranial tumor and it commonly spreads by direct extension and infiltration into the adjacent brain tissue and along the white matter tract. The metastatic spread of GBM outside of the central nervous system (CNS) is rare. The possible mechanisms of extraneural metastasis of the GBM have been suggested. They include the lymphatic spread, the venous invasion and the direct invasion through dura and bone. We experienced a 46-year-old man who had extraneural metastasis of the GBM on his left neck. The patient was treated with surgery for 5 times, radiotherapy and chemotherapy. He had survived 6 years since first diagnosed. Although the exact mechanism of the extraneural metastasis is not well understood, this present case shows the possibility of extraneural metastasis of the GBM, especially in patients with long survival.
Figure
-
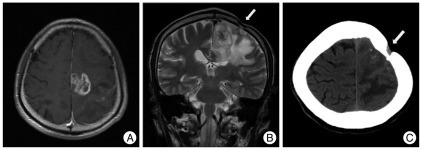
Fig. 1 Preoperative gadolinium enhanced T1-weighted magnetic resonance image (MRI) demonstrates a mass lesion with peripheral irregular well enhancement in the left parietal region (A). Preoperative T2-weighted coronal MRI (B) and computed tomography scan (C) show bony defect (arrow) suggesting previous craniotomy near the mass lesion.
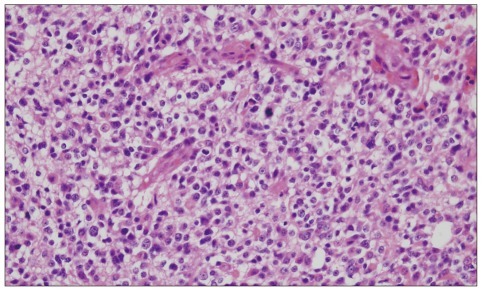
Fig. 2 Histologic findings after first operation show pleomorphic astrocytic tumor cells with mitosis and nuclear atypia (hematoxylin-eosin, original magnification, ×400).
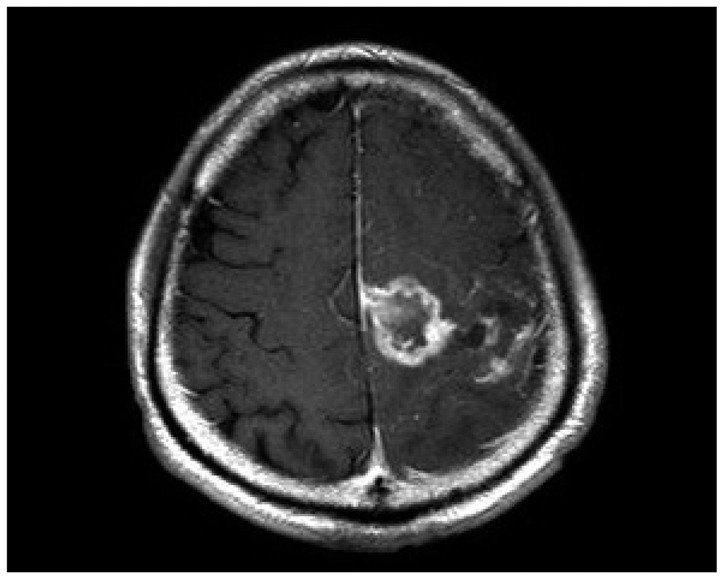
Fig. 3 Contrast enhanced magnetic resonance images taken 2 weeks after the first surgery shows remnant mass lesion in the parietal region.
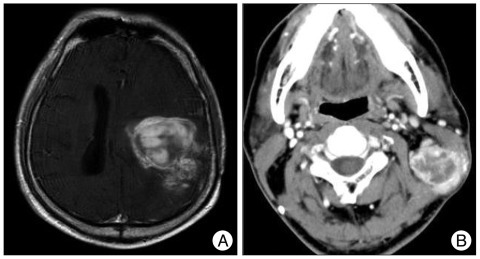
Fig. 4 A : Three-year follow up contrast enhanced magnetic resonance image shows increased enhancing mass of the left parietal lobe. B : The neck CT scan with contrast enhancement reveals new peripheral enhancing lesion with lymph node enlargement in the left neck. CT : computed tomography.
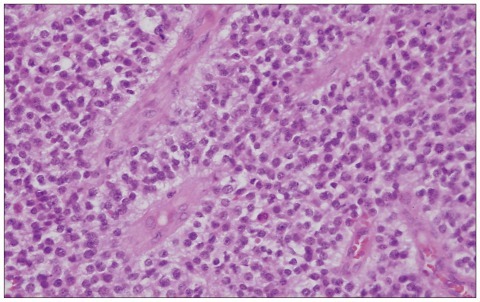
Fig. 5 Pathological specimen from the neck reveals increased cellularity, with blood vessel proliferation and necrosis (hematoxylin-eosin, original magnification, ×400).
Reference
-
1. Bernstein JJ, Woodard CA. Glioblastoma cells do not intravasate into blood vessels. Neurosurgery. 1995; 36:124–132. discussion 132. PMID: 7708148.
Article2. Cervio A, Piedimonte F, Salaberry J, Alcorta SC, Salvat J, Diez B, et al. Bone metastases from secondary glioblastoma multiforme : a case report. J Neurooncol. 2001; 52:141–148. PMID: 11508813.3. Giese A, Loo MA, Rief MD, Tran N, Berens ME. Substrates for astrocytoma invasion. Neurosurgery. 1995; 37:294–301. discussion 301-302. PMID: 7477782.
Article4. Hsu E, Keene D, Ventureyra E, Matzinger MA, Jimenez C, Wang HS, et al. Bone marrow metastasis in astrocytic gliomata. J Neurooncol. 1998; 37:285–293. PMID: 9524086.5. Huang P, Allam A, Taghian A, Freeman J, Duffy M, Suit HD. Growth and metastatic behavior of five human glioblastomas compared with nine other histological types of human tumor xenografts in SCID mice. J Neurosurg. 1995; 83:308–315. PMID: 7616277.
Article6. Liwnicz BH, Rubinstein LJ. The pathways of extraneural spread in metastasizing gliomas : a report of three cases and critical review of the literature. Hum Pathol. 1979; 10:453–467. PMID: 381159.7. Mentrikoski M, Johnson MD, Korones DN, Scott GA. Glioblastoma multiforme in skin : a report of 2 cases and review of the literature. Am J Dermatopathol. 2008; 30:381–384. PMID: 18645311.
Article8. Moon KS, Jung S, Lee MC, Kim IY, Kim HW, Lee JK, et al. Metastatic glioblastoma in cervical lymph node after repeated craniotomies : report of a case with diagnosis by fine needle aspiration. J Korean Med Sci. 2004; 19:911–914. PMID: 15608410.
Article9. Pansera F, Pansera E. An explanation for the rarity of extraaxial metastases in brain tumors. Med Hypotheses. 1992; 39:88–89. PMID: 1435399.
Article10. Pasquier B, Lachard A, Pasquier D, Muller F, Couderc P, Courel-Vidard MN, et al. [Costal micrometastasis from a cerebral astrocytoma. Immunohistochemical detection (author's transl)]. Arch Anat Cytol Pathol. 1982; 30:50–55. PMID: 6282226.11. Pasquier B, Pasquier D, N'Golet A, Panh MH, Couderc P. Extraneural metastases of astrocytomas and glioblastomas : clinicopathological study of two cases and review of literature. Cancer. 1980; 45:112–125. PMID: 6985826.
Article12. Rajagopalan V, El Kamar FG, Thayaparan R, Grossbard ML. Bone marrow metastases from glioblastoma multiforme--a case report and review of the literature. J Neurooncol. 2005; 72:157–161. PMID: 15925996.
Article13. Stark AM, Nabavi A, Mehdorn HM, BlÖmer U. Glioblastoma multiforme-report of 267 cases treated at a single institution. Surg Neurol. 2005; 63:162–169. discussion 169. PMID: 15680662.
Article14. Subramanian A, Harris A, Piggott K, Shieff C, Bradford R. Metastasis to and from the central nervous system--the 'relatively protected site'. Lancet Oncol. 2002; 3:498–507. PMID: 12147436.
Article15. Wallace CJ, Forsyth PA, Edwards DR. Lymph node metastases from glioblastoma multiforme. AJNR Am J Neuroradiol. 1996; 17:1929–1931. PMID: 8933881.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Meningioma Compatible with Metastatic Glioblastoma Multiforme
- A Case of Multicentric Glioblastoma Multiforme
- Scalp Metastasis of Glioblastoma Multiforme after Craniotomy and stereotatic Interstitial Brachytherapy
- Glioblastoma Multiforme with Initially Presenting Massive Intracranial Hemorrhage
- Comparison of Solitary Cerebral Metastasis and Glioblastoma Multiforme
