A Morphologically Atypical Case of Atlantoaxial Rotatory Subluxation
- Affiliations
-
- 1Department of Neurosurgery, Nagoya University School of Medicine, Nagoya, Japan. umebayad@gmail.com
- KMID: 2018036
- DOI: http://doi.org/10.3340/jkns.2014.55.5.284
Abstract
- A rare case of atlantoaxial rotatory subluxation occurred after pediatric cervical spine surgery performed to remove a dumbbell-shaped meningioma at the level of the C1/C2 vertebrae. This case is classified as a post-surgical atlantoaxial rotatory subluxation, but has a very rare morphology that has not previously been reported. Although there are several reports about post-surgical atlantoaxial rotatory subluxation, an important point of this case is that it might be directly related to the spinal cord surgery in C1/C2 level. On day 6 after surgery, the patient presented with the Cock Robin position, and a computed tomography scan revealed a normal type of atlantoaxial rotatory subluxation. Manual reduction was performed followed by external fixation with a neck collar. About 7 months after the first surgery, the subluxation became severe, irreducible, and assumed an atypical form where the anterior tubercle of C1 migrated to a cranial position, and the posterior tubercle of C1 and the occipital bone leaned in a caudal direction. The pathogenic process suggested deformity of the occipital condyle and bilateral C2 superior facets with atlantooccipital subluxation. A second operation for reduction and fixation was performed, and the subluxation was stabilized by posterior fixation. We encountered an unusual case of a refractory subluxation that was associated with an atypical deformity of the upper spine. The case was successfully managed by posterior fixation.
Figure
-

Fig. 1 Magnetic resonance imaging (MRI). A : Sagittal T1 weighted image. B : Sagittal T1 weighted image with gadolinium enhancement. C : Coronal T1 weighted image with gadolinium enhancement. D : Axial T1 weighted image with gadolinium enhancement at upper rim of C1 level. E : Axial T1 weighted image with gadolinium enhancement at lower rim of C1 level. The tumor seems to be intradural extramedurally tumor without dural tail sign, and its shape is semiovale. The tumor is iso signal intensity in T1 weighted image, and homogenously enhanced with gadolinium (B-E). These images show a dumbbell shaped spinal tumor, which is intradural extramedullary tumor at right foramen of C2 root (C). It is located in the right side of the spinal canal at C1/2 level and spinal cord is deviated to left due to the compression of tumor (D and E).

Fig. 2 A : Plain radiograph of the cervical spine shows an atypical form of subluxation in which the anterior tubercle of C1 had migrated to a cranial position, the posterior tubercle of C1 had migrated in a caudal direction, and the occipital bone began to lean caudally. B : The postoperative radiograph shows occipital plate C2-C3-C4 bilateral screw fixation and recovery of cervical lordosis.

Fig. 3 Computed tomography images of the cervical spine. A : Sagittal image showing the kyphotic cervical alignment. B : Axial images showing that the Fielding classification was type 1.
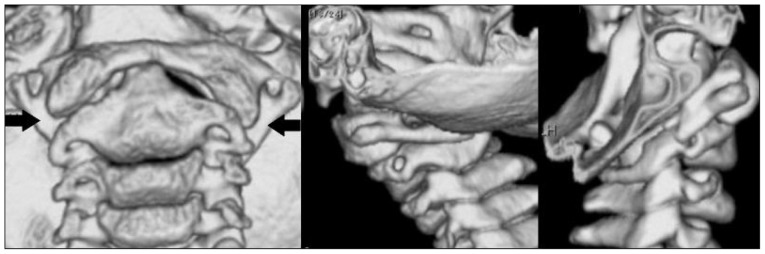
Fig. 4 Three-dimensional computed tomography images of the cervical spine show deformities of the C2 superior facet (arrow), and that the C1 vertebra was rotated to the left.
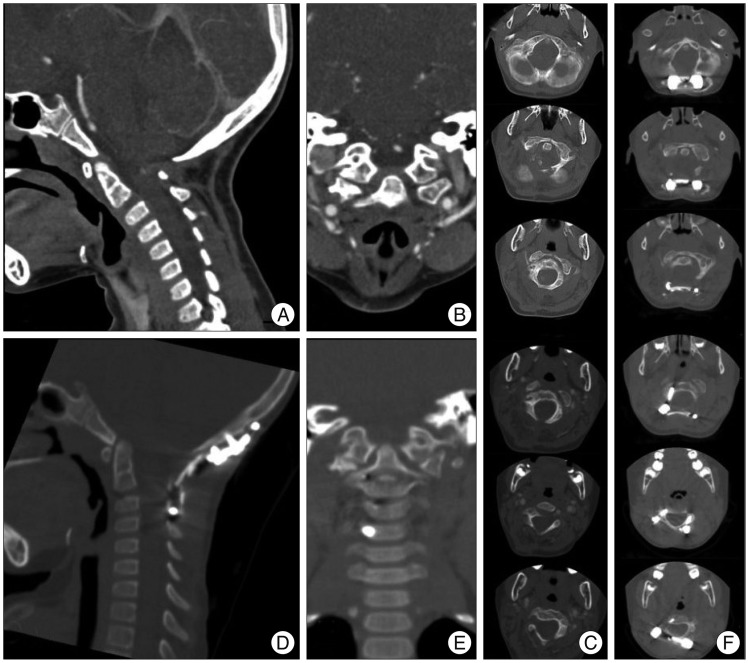
Fig. 5 A, B, and C : Pre-operative computed tomography images. D, E, and F : Postoperative computed tomography images of the cervical spine. Screws are inserted correctly and posterior fixation is achieved. Alignment is recovered.
Reference
-
1. Doshi J, Anari S, Zammit-Maempel I, Paleri V. Grisel syndrome : a delayed presentation in an asymptomatic patient. J Laryngol Otol. 2007; 121:800–802. PMID: 17295941.2. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977; 59:37–44. PMID: 833172.
Article3. Hamai S, Harimaya K, Maeda T, Hosokawa A, Shida J, Iwamoto Y. Traumatic atlanto-occipital dislocation with atlantoaxial subluxation. Spine (Phila Pa 1976). 2006; 31:E421–E424. PMID: 16741443.
Article4. Ishii K, Chiba K, Maruiwa H, Nakamura M, Matsumoto M, Toyama Y. Pathognomonic radiological signs for predicting prognosis in patients with chronic atlantoaxial rotatory fixation. J Neurosurg Spine. 2006; 5:385–391. PMID: 17120886.
Article5. Ishii K, Toyama Y, Nakamura M, Chiba K, Matsumoto M. Management of chronic atlantoaxial rotatory fixation. Spine (Phila Pa 1976). 2012; 37:E278–E285. PMID: 22281477.
Article6. Pang D. Atlantoaxial rotatory fixation. Neurosurgery. 2010; 66(3 Suppl):161–183. PMID: 20173520.
Article7. Pilge H, Prodinger PM, Bürklein D, Holzapfel BM, Lauen J. Nontraumatic subluxation of the atlanto-axial joint as rare form of acquired torticollis : diagnosis and clinical features of the Grisel's syndrome. Spine (Phila Pa 1976). 2011; 36:E747–E751. PMID: 21178843.8. Subach BR, McLaughlin MR, Albright AL, Pollack IF. Current management of pediatric atlantoaxial rotatory subluxation. Spine (Phila Pa 1976). 1998; 23:2174–2179. PMID: 9802157.
Article9. Wilson BC, Jarvis BL, Haydon RC 3rd. Nontraumatic subluxation of the atlantoaxial joint : Grisel's syndrome. Ann Otol Rhinol Laryngol. 1987; 96:705–708. PMID: 3688763.
Article10. Wilson MJ, Michele AA, Jacobson EW. Spontaneous dislocation of the atlanto-axial articulation, including a report of a case with quadriplegia. J Bone Joint Surg Am. 1940; 22:698–707.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Atlantoaxial Rotatory Fixation and Unilateral Counter Occipitoatlantal Subluxation after Minor Trauma
- Torticollis and Atlantoaxial Rotatory Subluxation after Chiropractic Therapy
- A Spontaneous Atlantoaxial Subluxation: A case repor
- Role of the O-arm and Computer-assisted Navigation of Safe Screw Fixation in Children with Traumatic Rotatory Atlantoaxial Subluxation
- The Treatment of Traumatic Atlantoaxial Rotatory Subluxation (Fielding Type I) and the Correlation between the Clinical Progress and Radiological Reduction Parameter
