Long-term implant success at the Academy for Oral Implantology: 8-year follow-up and risk factor analysis
- Affiliations
-
- 1Academy for Oral Implantology, Vienna, Austria. pommer@implantatakademie.at
- KMID: 2012984
- DOI: http://doi.org/10.5051/jpis.2014.44.3.102
Abstract
- PURPOSE
Rehabilitation of the incomplete dentition by means of osseointegrated dental implants represents a highly predictable and widespread therapy; however, little is known about potential risk factors that may impair long-term implant success.
METHODS
From 2004 to 2012, a total of 13,147 implants were placed in 4,316 patients at the Academy for Oral Implantology in Vienna. The survival rates after 8 years of follow-up were computed using the Kaplan-Meier method, and the impact of patient- and implant-related risk factors was assessed.
RESULTS
Overall implant survival was 97% and was not associated with implant length (P=0.930), implant diameter (P=0.704), jaw location (P=0.545), implant position (P=0.450), local bone quality (P=0.398), previous bone augmentation surgery (P=0.617), or patient-related factors including osteoporosis (P=0.661), age (P=0.575), or diabetes mellitus (P=0.928). However, smoking increased the risk of implant failure by 3 folds (P<0.001) and a positive history of periodontal disease doubled the failure risk (P=0.001).
CONCLUSIONS
Summing up the long-term results of well over 10,000 implants at the Academy for Oral Implantology in Vienna it can be concluded that there is only a limited number of patients that do not qualify for implant therapy and may thus not benefit from improved quality of life associated with fixed implant-retained prostheses.
Keyword
MeSH Terms
Figure
-
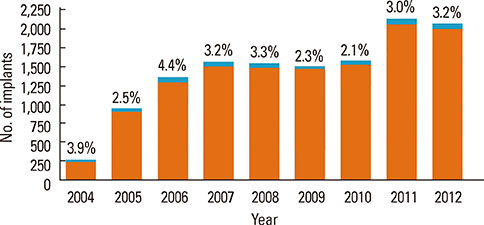
Figure 1 The number of dental implants placed at the Academy for Oral Implantology increased significantly in the years 2004 to 2012 (over 2000 implants per year) while the failure rate remained stable at around 3%.
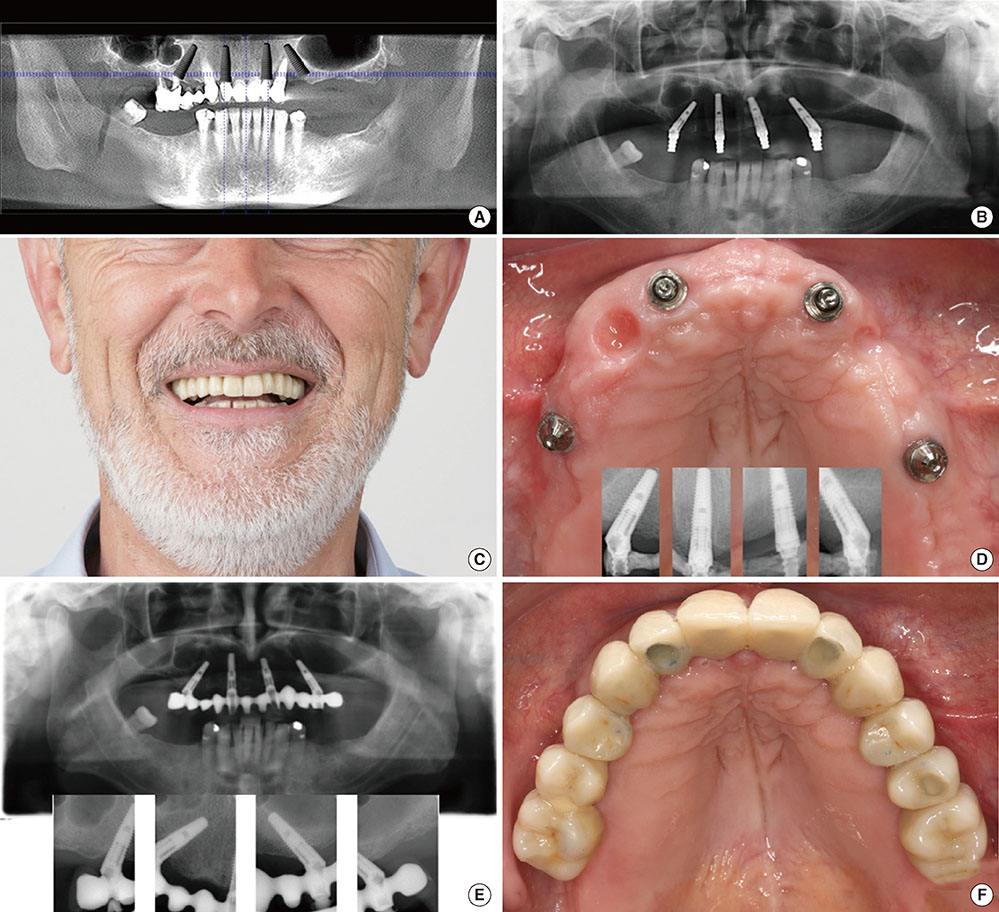
Figure 2 Implant rehabilitation of the completely edentulous maxilla according to the All-on-4 (Nobel Biocare, Gothenburg, Sweden) flapless protocol. (A) Preoperative planning procedure using cone-beam computed tomographic scans, (B) postoperative x-ray with impression copings and angulated multiunit abutments on tilted distal implants, (C) immediate temporary fixed restoration delivered at the day of surgery, (D) pictures and x-rays at final prosthesis delivery, and (E, F) 5 years after implant placement.
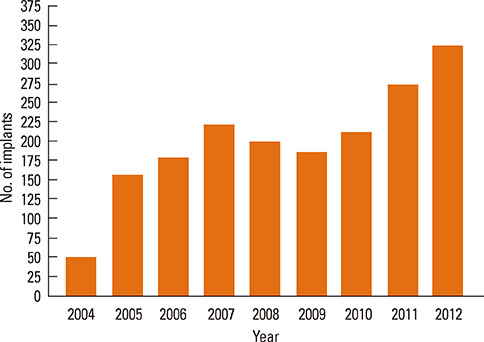
Figure 3 The number of grafting procedures to enhance bone volume for implant insertion (total of 1,917 sinus floor elevation operations, horizontal or vertical block augmentations, and socket grafts).
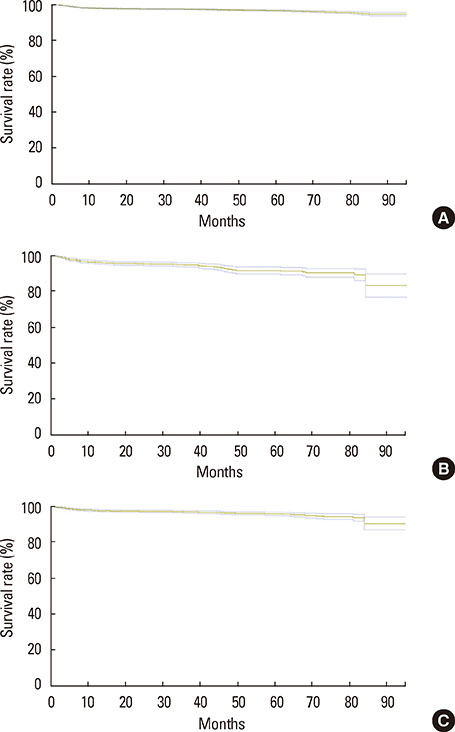
Figure 4 Kaplan-Meier curves (and 95% confidence intervals) for implant survival through 96 months (8 years) in healthy patients (A), smokers (B), and patients suffering periodontal disease (C).
Cited by 2 articles
-
The feasibility of immediately loading dental implants in edentulous jaws
Anders Henningsen, Ralf Smeets, Aria Wahidi, Lan Kluwe, Frank Kornmann, Max Heiland, Till Gerlach
J Periodontal Implant Sci. 2016;46(4):234-243. doi: 10.5051/jpis.2016.46.4.234.Risk indicators related to peri-implant disease: an observational retrospective cohort study
Pier Paolo Poli, Mario Beretta, Giovanni Battista Grossi, Carlo Maiorana
J Periodontal Implant Sci. 2016;46(4):266-276. doi: 10.5051/jpis.2016.46.4.266.
Reference
-
1. Pommer B, Zechner W, Watzek G, Palmer R. To graft or not to graft? Evidence-based guide to decision making in oral bone graft surgery. In : Zorzi A, Miranda J, editors. Bone Grafting. Rijeka: InTech;2012. p. 159–182.2. Levin L. Dealing with dental implant failures. J Appl Oral Sci. 2008; 16:171–175.
Article3. Palma-Carrio C, Maestre-Ferrín L, Penarrocha-Oltra D, Penarrocha-Diago MA, Penarrocha-Diago M. Risk factors associated with early failure of dental implants: a literature review. Med Oral Patol Oral Cir Bucal. 2011; 16:e514–e517.
Article4. Lee JH, Frias V, Lee KW, Wright RF. Effect of implant size and shape on implant success rates: a literature review. J Prosthet Dent. 2005; 94:377–381.
Article5. Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 2006; 17:Suppl 2. 136–159.
Article6. Pommer B, Hof M, Fadler A, Gahleitner A, Watzek G, Watzak G. Primary implant stability in the atrophic sinus floor of human cadaver maxillae: impact of residual ridge height, bone density, and implant diameter. Clin Oral Implants Res. 2014; 25:e109–e113.
Article7. Diz P, Scully C, Sanz M. Dental implants in the medically compromised patient. J Dent. 2013; 41:195–206.
Article8. Clementini M, Rossetti PH, Penarrocha D, Micarelli C, Bonachela WC, Canullo L. Systemic risk factors for peri-implant bone loss: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2014; 43:323–334.
Article9. Pommer B, Frantal S, Willer J, Posch M, Watzek G, Tepper G. Impact of dental implant length on early failure rates: a meta-analysis of observational studies. J Clin Periodontol. 2011; 38:856–863.
Article10. Andersen E, Saxegaard E, Knutsen BM, Haanaes HR. A prospective clinical study evaluating the safety and effectiveness of narrow-diameter threaded implants in the anterior region of the maxilla. Int J Oral Maxillofac Implants. 2001; 16:217–224.11. Polizzi G, Rangert B, Lekholm U, Gualini F, Lindstrom H. Branemark System Wide Platform implants for single molar replacement: clinical evaluation of prospective and retrospective materials. Clin Implant Dent Relat Res. 2000; 2:61–69.
Article12. Arisan V, Bolukbasi N, Ersanli S, Ozdemir T. Evaluation of 316 narrow diameter implants followed for 5-10 years: a clinical and radiographic retrospective study. Clin Oral Implants Res. 2010; 21:296–307.
Article13. Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971; 26:266–279.
Article14. Lekholm U, Zarb GA. Patient selection and preparation. In : Branemark PI, Zarb GA, Albrektsson T, editors. Tissue-integrated prostheses: osseointegration in clinical dentistry. Chicago: Quintessence;1985. p. 199–220.15. Charyeva O, Altynbekov K, Zhartybaev R, Sabdanaliev A. Long-term dental implant success and survival: a clinical study after an observation period up to 6 years. Swed Dent J. 2012; 36:1–6.16. Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success: a 10-16-year follow-up of non-submerged dental implants. Clin Oral Implants Res. 2010; 21:772–777.
Article17. Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002; 29:Suppl 3. 197–212.
Article18. Monje A, Chan HL, Fu JH, Suarez F, Galindo-Moreno P, Wang HL. Are short dental implants (<10 mm) effective? A meta-analysis on prospective clinical trials. J Periodontol. 2013; 84:895–904.
Article19. Sohrabi K, Mushantat A, Esfandiari S, Feine J. How successful are small-diameter implants? A literature review. Clin Oral Implants Res. 2012; 23:515–525.
Article20. Strietzel FP, Reichart PA, Kale A, Kulkarni M, Wegner B, Kuchler I. Smoking interferes with the prognosis of dental implant treatment: a systematic review and meta-analysis. J Clin Periodontol. 2007; 34:523–544.
Article21. Safii SH, Palmer RM, Wilson RF. Risk of implant failure and marginal bone loss in subjects with a history of periodontitis: a systematic review and meta-analysis. Clin Implant Dent Relat Res. 2010; 12:165–174.
Article22. Bornstein MM, Cionca N, Mombelli A. Systemic conditions and treatments as risks for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:Suppl. 12–27.23. Salvi GE, Carollo-Bittel B, Lang NP. Effects of diabetes mellitus on periodontal and peri-implant conditions: update on associations and risks. J Clin Periodontol. 2008; 35:8 Suppl. 398–409.
Article24. Chao YL, Chen HH, Mei CC, Tu YK, Lu HK. Meta-regression analysis of the initial bone height for predicting implant survival rates of two sinus elevation procedures. J Clin Periodontol. 2010; 37:456–465.
Article25. Esposito M, Grusovin MG, Rees J, Karasoulos D, Felice P, Alissa R, et al. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev. 2010; (3):CD008397.
Article26. Graziani F, Donos N, Needleman I, Gabriele M, Tonetti M. Comparison of implant survival following sinus floor augmentation procedures with implants placed in pristine posterior maxillary bone: a systematic review. Clin Oral Implants Res. 2004; 15:677–682.
Article27. Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodontol. 2008; 35:8 Suppl. 216–240.
Article28. Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007; 22:Suppl. 49–70.29. Bernstein S, Cooke J, Fotek P, Wang HL. Vertical bone augmentation: where are we now? Implant Dent. 2006; 15:219–228.
Article30. Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry. Int J Oral Maxillofac Implants. 2009; 24:Suppl. 237–259.31. Clementini M, Morlupi A, Canullo L, Agrestini C, Barlattani A. Success rate of dental implants inserted in horizontal and vertical guided bone regenerated areas: a systematic review. Int J Oral Maxillofac Surg. 2012; 41:847–852.
Article32. Donos N, Mardas N, Chadha V. Clinical outcomes of implants following lateral bone augmentation: systematic assessment of available options (barrier membranes, bone grafts, split osteotomy). J Clin Periodontol. 2008; 35:8 Suppl. 173–202.
Article33. Jensen SS, Terheyden H. Bone augmentation procedures in localized defects in the alveolar ridge: clinical results with different bone grafts and bone-substitute materials. Int J Oral Maxillofac Implants. 2009; 24:Suppl. 218–236.34. Rocchietta I, Fontana F, Simion M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: a systematic review. J Clin Periodontol. 2008; 35:8 Suppl. 203–215.
Article35. Waasdorp J, Reynolds MA. Allogeneic bone onlay grafts for alveolar ridge augmentation: a systematic review. Int J Oral Maxillofac Implants. 2010; 25:525–531.36. Sbordone L, Toti P, Menchini-Fabris G, Sbordone C, Guidetti F. Implant survival in maxillary and mandibular osseous onlay grafts and native bone: a 3-year clinical and computerized tomographic follow-up. Int J Oral Maxillofac Implants. 2009; 24:695–703.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Criteria for Dental Implant Success: A Systematic Literature Review
- Implant Placement on a Cementoosseous Dysplastic Mandible with a Long-term Follow-up: A Case Report
- Surgical Removal of Dental Implants Dislocated Into the Mandibular Body
- Horizontal ridge augmentation with porcine bone-derived grafting material: a long-term retrospective clinical study with more than 5 years of follow-up
- Retrospective Observational Study of Narrow Diameter Implants
